Inspired by Huang et al 2024.[1]
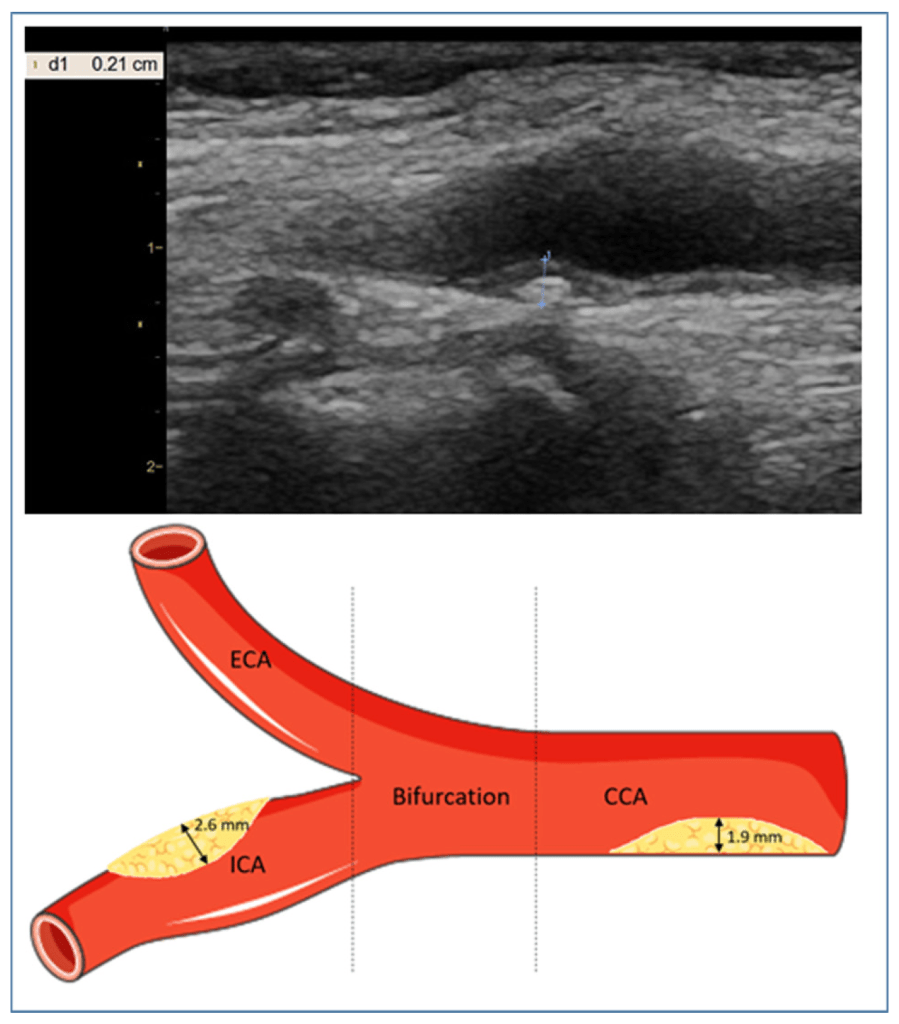
Calculation of carotid plaque score.
CAD – carotid atherosclerotic disease
US – ultrasound
SCM – sternocleidomastoid (muscle)
cIMT – carotid intima-media thickness
PS – plaque score (based on plaque thickness)
PV – plaque volume (3D measure)
GSM – grey-scale median (3D measure of fibrosis and hence plaque stability)
PWV – pulse wave velocity
BS – beginning of systole (timing of PWV measurement)
ES – end of systole (timing of PWV measurement)
SD – standard deviation– key to acronyms
We have another paper from Huang et al this week, but this Huang comes from Guangzhou, China rather than Taichung City, Taiwan. There is another link though. Last week we discussed stroke risk in insomnia, and there was some discussion at the blog webinar about statins and (atherosclerotic) plaque stability. I made a mental note to look up the data on this, and before I got a chance, the current paper popped up, so my choice this week was easy.
This is the first trial to examine the effects of acupuncture on US measurements of asymptomatic carotid atherosclerosis (CAD). It is a relatively small trial with just 55 completing the 12-week, 24 session treatment course. Initially, 60 were randomised to real acupuncture or non-penetrating sham acupuncture. 2 dropped out of the real acupuncture group and 3 from the sham group.
The points used were ST9, Yintang, GV20, PC6, GB34. I think this is the first time I have ever discussed ST9. Whilst we often needle the SCM muscle close to this point, we clearly never approach the medial aspect of the carotid. Bob Gerwin did teach me how to needle longus colli in the neck by pushing the larynx to one side and going directly AP onto the vertebral bodies of the mid cervical spine. This approach does go medial to the common carotid artery, but not as close as the point ST9. I only ever performed this technique once in a patient who suffered chronic myofascial pain in the anterior neck secondary to a rotational squint in childhood. It was at the specific request of the patient who had his own copy of the Trigger Point Manual by Travell and Simons.
ST9 is at the level of the laryngeal prominence and medial to the SCM. In this paper they describe needling at the fluctuation site of the common carotid artery, but only to a depth of 5 to 10mm. Other references describe needling 0.5 to 1 cun, which is twice as far, but also mention deliberately holding the artery to the side (laterally). So, the intention is clearly to get close, but not too close.
The primary outcome measures were US measures of carotid artery structure: cIMT, PS, PV, GSM. The secondary measures were of pulse wave velocity (PWV) at different times (BS and ES). These were measured on 3 occasions: baseline, 12 weeks (after treatment phase), and 24 weeks (12 weeks post treatment).
Plaque score (PS) is a strong predictor of ischaemic stroke and major adverse cardiovascular events (MACE – this acronym has figured on the blog previously).[2]
There were significant differences between groups in PS following the treatment phase and at the later follow-up. It is hard to interpret these, as they are expressed in millimetres change, whereas the PS is usually a numerical score based on the thickness of the thickest plaques in 4 different regions of the carotid: common portion, bifurcation, external, internal. It looks as though the biggest change was just under 0.5mm, which may not be enough to change the standard numerical score where the difference between each number is 1mm of plaque thickness. Anyway, it is the right direction, and it gets me thinking about possible mechanisms, and whether or not it is really necessary to needle close to the artery in first place.
PV reduced by just over 23mm3 in the acupuncture group compared with less than 3mm3 in the sham group. Whilst this was highly significant statistically, the distributions here were quite different in size with the SD in the acupuncture group being over 6 times larger than that in the sham group. This indicates that some individuals did a lot better than some others.
In terms of plaque stability, as measured by GSM, there was a significant difference between groups following the treatment phase, but this dropped to a trend only at follow-up due to a minor catch up in the sham group.
There were no significant differences in the measures of arterial wall thickness (cIMT) or PWV.
I thought I better have a quick look at the data on statins for some sort of comparison. There is a lot of data, but most of it is funded by industry, and much of it uses surrogate outcomes, just like the ones measured above.
Rather than wade through this mass of data, I narrowed things down by just looking at the Cochrane Database of Systematic Reviews. There are a surprising number of these with statins in the title. I found one from last year examining pharmacological interventions for asymptomatic carotid stenosis. This is a very similar population, but probably with more severe CAD than the current trial population, as it focussed on internal carotid stenosis rather than just the presence of CAD. There was no evidence for reduction of strokes or stroke-related mortality from lipid-lowering agents (all statins), although there seemed to be a trend in favour of them.[3]
I thought I better look for some positive data for statins on the Cochrane Database, and sure enough there was a positive review published in 2013 with the title Statins for the primary prevention of cardiovascular disease.[4] There was a lot more data in this review (over 48k patients) than the one focussing on carotid stenosis and a clear reduction in mortality of just under 15%. All the data in this meta-analysis came from trials funded by the pharmaceutical industry.
The huge retrospective observational cohorts are not the same as meta-analysis of prospective industry-funded trials; however, just for speculative counter point, the reduction in all-cause mortality associated with acupuncture in a hypertensive population was 27% (see: Acupuncture and MACE).
Finally, I was surprised to find that I have actually mentioned atheroma on the blog previously – way back in 2019, with the rather unimaginative title of Atheroma 2019.
References
1 Huang X, Meng L, Zhao L, et al. Efficacy of acupuncture in patients with carotid atherosclerosis: a randomized controlled clinical trial. BMC Complement Med Ther. 2024;24:313. doi: 10.1186/s12906-024-04601-3
2 Ihle-Hansen H, Vigen T, Berge T, et al. Carotid Plaque Score for Stroke and Cardiovascular Risk Prediction in a Middle-Aged Cohort From the General Population. J Am Heart Assoc. 2023;12:e030739. doi: 10.1161/JAHA.123.030739
3 Clezar CN, Flumignan CD, Cassola N, et al. Pharmacological interventions for asymptomatic carotid stenosis. Cochrane Database Syst Rev. 2023;8:CD013573. doi: 10.1002/14651858.CD013573.pub2
4 Taylor F, Huffman MD, Macedo AF, et al. Statins for the primary prevention of cardiovascular disease. Cochrane Database Syst Rev. 2013;2013:CD004816. doi: 10.1002/14651858.CD004816.pub5

You must be logged in to post a comment.