
Stimulated by Dunning et al 2025.[1]
EDN – electrical dry needling
OAK – OA knee
OA – osteoarthritis
IF – impact factor
PEDN – periosteal electrical dry needling
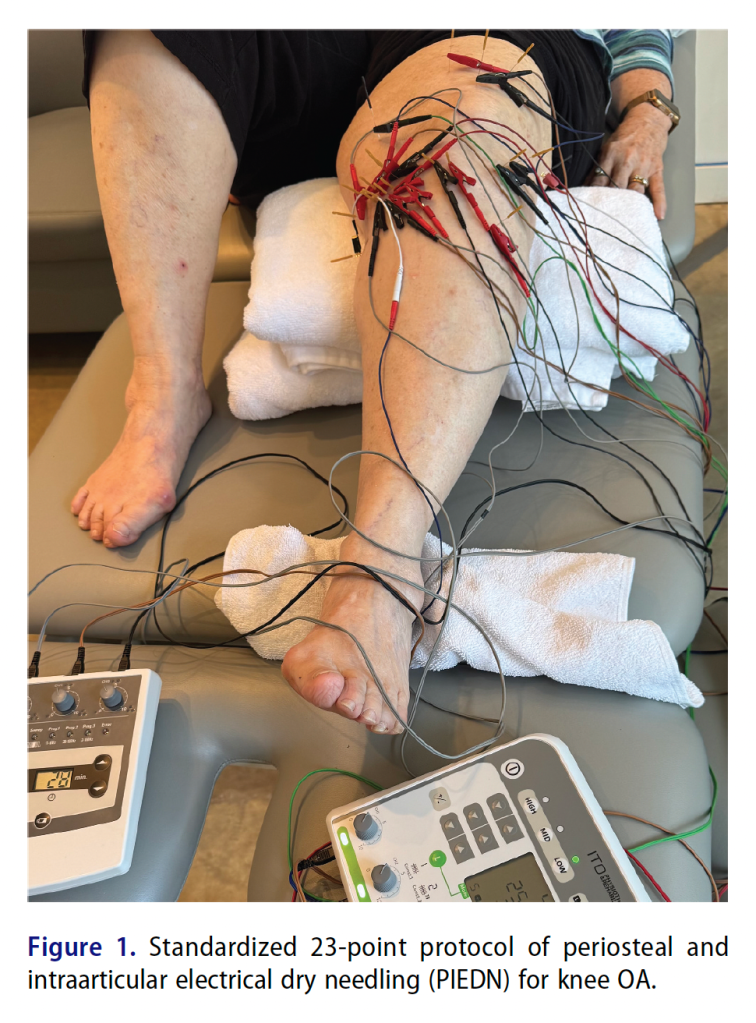
PIEDN – periosteal and intra-articular electrical dry needling
EA – electroacupuncture
WMA – Western medical acupuncture
TENS – transcutaneous electrical nerve stimulation
SAE – serious adverse event
WOMAC – Western Onterio and McMaster Universities osteoarthritis index
NPRS – numerical pain rating scale
GROC – global rating of change
MSK – musculoskeletal– key to acronyms
This paper was published online last month in the journal Physiotherapy Theory and Practice (IF 1.5). I have been meaning to mention it here, and was reminded to do so by a couple of colleagues from the US.
The term dry needling has been used for decades, and I think it was originally used to differentiate the needle effect from that of an injected substance in wet needling or injection techniques for pain. As long ago as 1979, Karel Lewit wrote about this in the journal of the same name (Pain).[2]
Dry needling used hypodermic needles initially, but most clinicians made the move to using the less traumatic solid filiform needles, which were designed for acupuncture. Chang-Zern Hong was an exception, as he favoured injection of tiny quantities of local anaesthetic with each thrust of his long 23G (blue) hypodermic needles. He demonstrated that this was associated with less post-needling soreness;[3] however, I don’t think he ever compared post-needling soreness following dry needling with a hypodermic needle and with an acupuncture needle. My guess is that the latter would be considerably less than the former.
Dry needling was mostly targeted at myofascial trigger points as an alternative to wet needling; however, some clinicians did start using dry needling techniques targeted at enthesopathies as well. Most recently, terminology has been expanding to include EDN, PEDN, and PIEDN. These are all essentially forms of EA, but in some countries, some health professions are not free to use the term acupuncture, so we have this rather confusing plethora of new acronyms.
Within traditional acupuncture, intra-articular needling has been performed for a long time (possibly for 2 millennia). A modern understanding of how acupuncture works combined with an appreciation of rare but catastrophic adverse events has led us (BMAS) to avoid intra-articular needling with acupuncture needles. Infection in joints and around prostheses following local acupuncture is very rare and occurs principally where the (usually) metal prosthesis is rather superficial,[4,5] or the joint space is close to the skin surface (in the anterior knee for example).[5–7]
I still meet many traditionally trained practitioners who are convinced that intra-articular needling is an essential part of their treatment of stiff knees, and the rarity of infection following acupuncture means that most will never see this complication. But from a WMA perspective, since there are almost no nerves within the joint space, there can be no benefit in penetrating the joint with a solid needle.
Moving on to periosteal acupuncture, this has been featured here before – see Periosteal techniques 1963-2018. It was developed by Felix Mann in about 1963, and he considered it one of the most important developments in his career.[8] Of course, this is a mechanical stimulus, as developed by Felix. Whilst the fibrous surface layer of periosteum is densely innervated, the deeper part is very sparsely innervated and cortical bone has no nerve endings. My impression is that when an acupuncture needle tip is embedded in periosteum, it is essentially insulated from the surroundings. Because of the shape of the needle tip, its surface area to volume ratio is approximately double that of the needle shaft, so the electric field generated around it during an EA pulse is also greater. If the tip is in periosteum, there is no advantage in terms of nerve stimulation, so patients tend to feel the most sensitive nerves along the shaft, which is usually the large fibres in the skin. Essentially, this means that applying EA after periosteal needling is probably similar to applying TENS.
I hope I have argued adequately that PEDN and PIEDN do not add much to the mechanical stimulus of periosteal needling, and in the case of PIEDN, add a small risk of an SAE.
Having said all that, and despite my reservations about the techniques used in this paper, there is still something to gain from the data. It is a large 3-arm trial (n=586) comparing different top-up regimes following 8 to 10 sessions of PIEDN over 6 weeks. The top-ups were either 4 weekly, 8 weekly, or none. The main outcome was the WOMAC total score. Secondary outcomes were NPRS, 3 WOMAC subscales, medication intake and GROC.
The MCID for the WOMAC total score is ~10 points on the 0-96 original version. All three groups improved by more than twice this in the first 6 weeks of treatment. By 14 weeks all three groups had continued to improve, but there was a trend appearing in favour of the 4 weekly top-up group. By 22 weeks (4 vs 2 vs 0 top-ups) the groups had diverged significantly, and they continued to diverge to the 30-week point.
Thankfully there were no SAEs reported in this trial, although almost 60% experienced post-needling soreness, and over 30% reported bruising.
Two decades ago, we set up a high volume acupuncture clinic (subsequently known as group acupuncture clinic) to perform a simple 4-point (per knee) EA protocol in OAK. There was an initial course of 8 sessions over 12 weeks (4 weekly then 4 fortnightly) followed by monthly top-ups.[9] The clinic was very successful and expanded to included other MSK conditions until the funding was pulled by commissioners.
References
1 Dunning J, Young I, Taylor N, et al. Effect of dose interval of periosteal and intraarticular electrical dry needling boosters on pain and disability in patients with knee osteoarthritis: a multi-center randomized clinical trial. Physiother Theory Pract. 2025;1–14. doi: 10.1080/09593985.2025.2575837
2 Lewit K. The needle effect in the relief of myofascial pain. Pain. 1979;6:83–90. doi: 10.1016/0304-3959(79)90142-8
3 Hong C-Z. Lidocaine injection versus dry needling to myofascial trigger point. The importance of the local twitch response. Am J Phys Med Rehabil. 1994;73:256–63. doi: 10.1097/00002060-199407000-00006
4 Kirschenbaum AE, Rizzo C. Glenohumeral pyarthrosis following acupuncture treatment. Orthopedics. 1997;20:1184–6. doi: 10.3928/0147-7447-19971201-15
5 Laing AJ, Mullett H, Gilmore MFX. Acupuncture-associated arthritis in a joint with an orthopaedic implant. J Infect. 2002;44:43–4. doi: 10.1053/jinf.2001.0911
6 Tien C-H, Huang G-S, Chang C-C, et al. Acupuncture-associated Listeria monocytogenes arthritis in a patient with rheumatoid arthritis. Joint Bone Spine. 2008;75:502–3. doi: 10.1016/j.jbspin.2007.08.010
7 Woo PCY, Lau SKP, Yuen K-Y. First report of methicillin-resistant Staphylococcus aureus septic arthritis complicating acupuncture: simple procedure resulting in most devastating outcome. Diagn Microbiol Infect Dis. 2009;63:92–5. doi: 10.1016/j.diagmicrobio.2008.08.023
8 Mann F. Reinventing Acupuncture: A New Concept of Ancient Medicine. 1st ed. Butterworth-Heinemann 1992.
9 Berkovitz S, Cummings M, Perrin C, et al. High Volume Acupuncture Clinic (Hvac) for Chronic Knee Pain – Audit of a Possible Model for Delivery of Acupuncture in the National Health Service. Acupunct Med. 2008;26:46–50. doi: 10.1136/aim.26.1.46

You must be logged in to post a comment.