Stimulated by Lester et al 2026.[1]
IF – impact factor
CD – cluster of differentiation (classification for surface antigens on white blood cells)– key to acronyms
I have been waiting a long time for an adverse event report of infection following acupuncture in a patient undergoing chemotherapy. We have been talking about this risk for decades,[2] yet this is the first report I have seen.
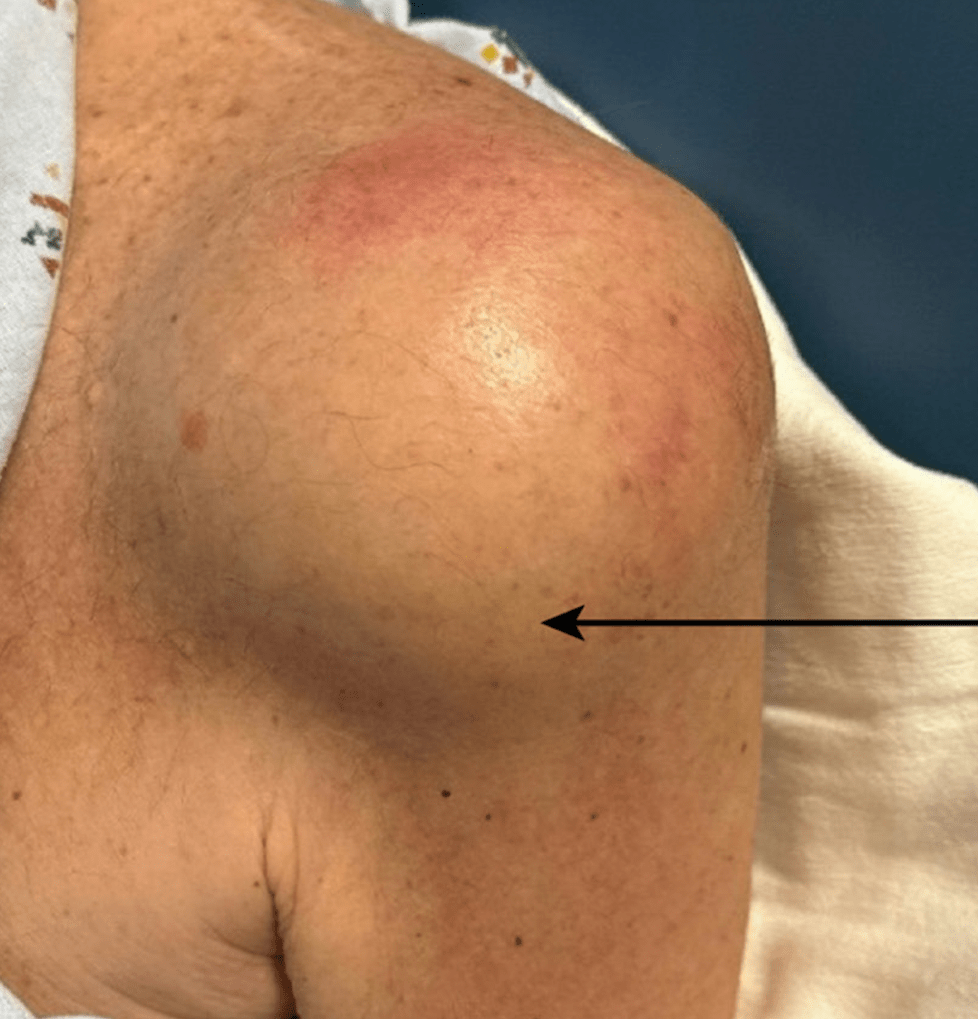
The report is published in the Americal Journal of Case Reports (IF 0.7) and involves a 69-year-old man undergoing chemotherapy for relapsed multiple myeloma. The acupuncture was performed along with physical therapy for chronic left shoulder pain and commenced about a month prior to his admission with an acute exacerbation of pain along with obvious swelling of his left shoulder.
The fluid in his subacromial and subdeltoid bursa was drained and grew Staphylococcus epidermidis, which was resistant to the antibiotics he happened to be taking prophylactically as well as several others.
The report mentions that he had been treated for Staphylococcus epidermidis bacteraemia the previous year, which rather complicates the otherwise relatively straightforward attribution of infection by inoculation from skin to subdeltoid bursa through acupuncture for chronic shoulder pain (probably at LI15). The distance from skin to bursa at LI15 in a slim shoulder is certainly within the inoculation range being under 20mm.
The patient’s recovery was complicated by antibiotic resistance and vancomycin-induced acute kidney injury. This was superimposed on chemotherapy-induced cardiomyopathy with an ejection fraction of 40%, chronic kidney disease, hypertension, pancytopenia, and a history of spinal fracture complicated by osteomyelitis. He had undergone stem cell transplantation 14 years before, presumably as part of treatment for his multiple myeloma.
Unfortunately, we do not know the details of his chemotherapy regime apart from the biologic teclistamab. The latter is a bispecific T-cell-redirecting monoclonal antibody that links cytotoxic T-cells (via CD3) to plasma cells. It has a significant infection risk.
This report includes references to several other cases of acupuncture linked infections, a few of which I did not have in my files. They include both cases of septic arthritis,[3–7] and one case of infection around a metal implant.[8]
They did miss several of the older cases that I listed in the previous blog, both infections of orthopaedic implants in the knee,[9,10] and joint infections following acupuncture.[9–16]
Where the joint or metalwork is relatively superficial, inoculation from the skin is certainly a possible mechanism. This would include the sternoclavicular joint,[5] the glenohumeral joint (which communicates with the subdeltoid bursa),[1,16] the sacroiliac joint (the posterior inferior aspect can be quite superficial),[3,15] and the knee joint.[6,9–12] In terms of inoculation onto implants, the joint line of the knee,[6,9,10] the shoulder, and rods on the dorsal aspect of the spine are all possible routes.[8]
Infections in facet joints and intervertebral discs are unlikely to result from direct inoculation and haematogenous spread seems much more likely.[4,7,13,14] The latter is only likely to derive from acupuncture if the latter actually results in local infection in or under the skin.
References
1 Lester PR, Murawska Baptista A, Tapia Stoll N, et al. Septic Arthritis Secondary to Acupuncture in an Immunocompromised Patient With Multiple Comorbid Conditions. Am J Case Rep. 2026;27:e948392. doi: 10.12659/AJCR.948392
2 Filshie J. Safety aspects of acupuncture in palliative care. Acupunct Med. 2001;19:117–22.
3 Tseng Y-C, Yang Y-S, Wu Y-C, et al. Infectious sacroiliitis caused by Staphylococcus aureus following acupuncture: a case report. Acupunct Med. 2014;32:77–80. doi: 10.1136/acupmed-2013-010457
4 Robinson A, Lind CRP, Smith RJ, et al. Atlanto-axial infection after acupuncture. BMJ Case Rep. 2015;2015:bcr2015212110. doi: 10.1136/bcr-2015-212110
5 Liu B-M, Wang T-L, Hung S. Sternoclavicular Septic Arthritis Caused by Acupuncture over the Posterior Neck. Eur J Case Rep Intern Med. 2015;2. doi: 10.12890/2015_000188
6 Kruse JP, Lewis RJ, Smith HL, et al. Acupuncture-Associated Mycobacterium goodii Infection of Prosthetic Knee Joint. Infect Dis Clin Pract. 2019;27:e1–2. doi: 10.1097/IPC.0000000000000669
7 Yang W, Xia S, Li L, et al. Methicillin-Resistant Staphylococcus aureus-Induced Discitis Following Acupuncture: A Case Report. Infect Drug Resist. 2024;17:5839–46. doi: 10.2147/IDR.S500762
8 Callan AK, Bauer JM, Martus JE. Deep Spine Infection After Acupuncture in the Setting of Spinal Instrumentation. Spine Deform. 2016;4:156–61. doi: 10.1016/j.jspd.2015.09.045
9 Narayana Murthy S, Srinivasan SH, Archunan M, et al. Prosthetic knee joint infection by an unusual organism following acupuncture treatment. Acupunct Med. 2021;39:571–2. doi: 10.1177/0964528421990661
10 Laing AJ, Mullett H, Gilmore MFX. Acupuncture-associated arthritis in a joint with an orthopaedic implant. J Infect. 2002;44:43–4. doi: 10.1053/jinf.2001.0911
11 Woo PCY, Lau SKP, Yuen K-Y. First report of methicillin-resistant Staphylococcus aureus septic arthritis complicating acupuncture: simple procedure resulting in most devastating outcome. Diagn Microbiol Infect Dis. 2009;63:92–5. doi: 10.1016/j.diagmicrobio.2008.08.023
12 Tien C-H, Huang G-S, Chang C-C, et al. Acupuncture-associated Listeria monocytogenes arthritis in a patient with rheumatoid arthritis. Joint Bone Spine. 2008;75:502–3. doi: 10.1016/j.jbspin.2007.08.010
13 Daivajna S, Jones A, O’Malley M, et al. Unilateral Septic Arthritis of a Lumbar Facet Joint Secondary to Acupuncture Treatment – a Case Report. Acupunct Med. 2004;22:152–5. doi: 10.1136/aim.22.3.152
14 Ishibe M, Inoue M, Saitou K. Septic arthritis of a lumbar facet joint due to pyonex. Arch Orthop Trauma Surg. 2001;121:90–2.
15 Lau S-M, Chou C-T, Huang C-M. Unilateral sacroiliitis as an unusual complication of acupuncture. Clin Rheumatol. 1998;17:357–8. doi: 10.1007/BF01451023
16 Kirschenbaum AE, Rizzo C. Glenohumeral pyarthrosis following acupuncture treatment. Orthopedics. 1997;20:1184–6. doi: 10.3928/0147-7447-19971201-15

You must be logged in to post a comment.