Stimulated by Zhang et al 2026.[1]
EA – electroacupuncture
IF – impact factor
WDR – wide dynamic range
SD – Sprague Dawley
CFA – complete Freund’s adjuvant (an oily antigenic mixture including heat-killed mycobacteria)
PWR – paw withdrawal threshold
AAV – adeno-associated virus
RVM – rostral ventromedial medulla
GABA – gamma amino butyric acid
ChR2 – channel rhodopsin 2 (cation influx ie depolarisation with 470nm light)
eNpHR3.0 – enhanced halorhodopsin 3.0 (chloride ion influx ie hyperpolarisation with 560nm to 590nm light)
Np – Natronomonous pharaonic (the source organism for the halorhodopsin above)
NRM – nucleus raphe magnus (serotoninergic cells dominate)
GiA – nucleus reticularis gigantocellularis alpha (mixed GABAergic and glutaminergic)
PGi – nucleus reticularis paragigantocellularis (as GiA above)– key to acronyms
This paper comes from Wuhan, China, with some links to Beijing, Harbin, Lanzhou, Nanchang, Yangzhou, and Zhanjiang, which covers nearly all corners of China. It is published in the Sage journal Molecular Pain (IF 2.8), which has been around for just over 20 years (Volume 1 was in 1995).
Professor Xianghong Jing is one of the corresponding authors, and the topic of this paper is related to two previous blogs highlighting work on WDR neurons from her research group (see Pre-EA on spinal WDRs and EA for muscle tenderness 2026 or just put WDR in the search box).[2,3]
This was an experimental study using male SD rats, an inflammatory muscle pain model in gastrocnemius created by CFA injection, and contralateral EA applied to ST36 as the therapeutic input.
EA was applied on day 3, 4, and 5 after the CFA injection. The EA was applied to a pair of needles at ST36 for 20 minutes under anaesthesia at 2/15Hz and 2mA with a pulse width of 0.5ms. A fancy stimulator for neuroscience experiments was used (STG4008) and so I guess a bipolar waveform was applied, although this is not mentioned in the paper.
Behavioural tests were applied in a blinded manner to assess ipsilateral regional mechanical hyperalgesia (von Frey filaments to the ipsilateral hind paw measuring PWT) and spontaneous pain (bilateral relative weight bearing on both hindlimbs).
These tests demonstrated a robust effect of CFA injection on regional mechanical hyperalgesia over the experimental period; however, the test for spontaneous pain was only markedly different between groups on day 3 (the first day of EA). So, day 3 was subsequently used for the neural recordings from WDN cell bodies in the ipsilateral lumbar dorsal horn.
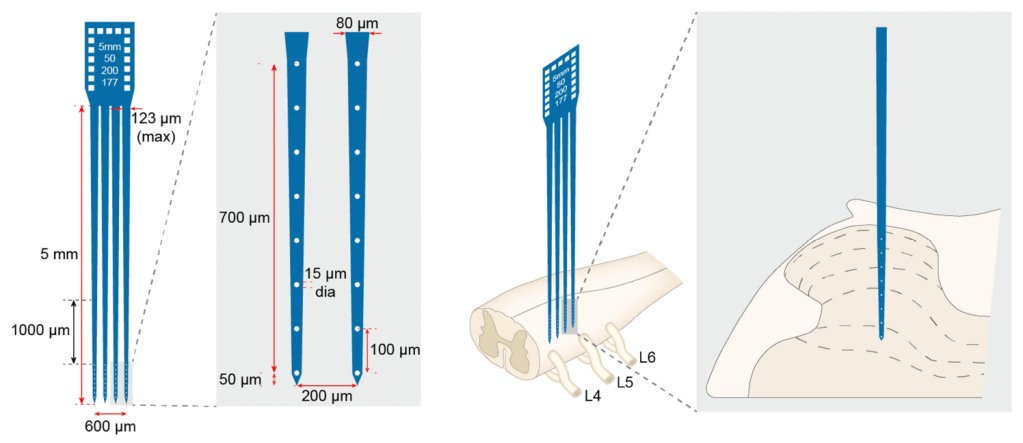
It sounds as though the recording from WDR cell bodies was performed in a similar way to previous experiments I have highlighted here using a sophisticated microelectrode array (see image in previous blogs Pre-EA on spinal WDRs and EA for muscle tenderness 2026).
WDR neurons were identified based on their responses to both non-noxious and noxious peripheral stimuli (60g or 200g pressure on the tender CFA-injected muscle with a blunt rubber probe). WDR nerve responses to 60g and 200g pressure on day 3 following CFA injection were both attenuated by EA.
Next neural tracing was used (both fluorogold and AAV tracers) to determine the descending fibres from the brainstem that might be responsible for this EA-mediated attenuation of WDR nerve activity. Roughly 75% of labelled nerves in the RVM (retrograde labelling from bilateral L4 to L6 segments) were also labelled as GABAergic.
These GABAergic neurons in the RVM were then subject to manipulation via AVVs containing genes for light sensitive channels (ChR2 or eNpHR3.0). Optogenic activation of GABAergic neurons in the RVM of naïve SD rats (ie without prior CFA injection) resulted in enhanced activation of WDR neurons in the lumbar dorsal horn following a 60g (non-noxious) stimulus but did not affect WDR activation following a 200g (noxious) stimulus. Optogenic inhibition of GABAergic neurons in the RVM resulted in reduced activation of WDR neurons in the lumbar dorsal horn to noxious stimulus but did not affect WDR activation following a non-noxious stimulus. Coherent results were found with behavioural testing (50% PWT) in naïve SD rats.
Simultaneous optogenic activation of GABAergic neurons in the RVM at the same time as contralateral EA stimulation in model SD rats resulted in attenuation of the effect of EA on mechanical hyperalgesia and weight-bearing. WDR responses were similarly affected with the expected reduction in WDR discharges following EA being attenuated or entirely absent through simultaneous activation of GABAergic neurons in the RVM.
The RVM has been prominent in the wiring diagrams of the analgesic mechanism of acupuncture since the 70’s and 80’s. The nuclei we used to talk about are now known as the NRM, GiA, and PGi, which are the sites of different descending systems of both inhibition and facilitation. The PAG drives some of this activity, particularly the acupuncture-mediated descending inhibition of nociception. We used to focus on β endorphin, serotonin, and noradrenalin, but know it looks as though we need to add GABA into the mix for consideration. Not as having an inhibitory influence on nociception in this case, but as an inhibitor of inhibitory spinal interneurons, which would result in nociceptive facilitation or in blocking of EA-mediated analgesia.
References
1 Zhang K, Yu Q, Yang Y, et al. Contralateral electroacupuncture modulates the transmission of nociceptive information in the spinal dorsal horn via GABAergic neurons in the rostral ventromedial medulla. Mol Pain. 2026;22:17448069261421426. doi: 10.1177/17448069261421426
2 Yu Q, Cao W, Wang X, et al. The Effect of Pre-Electroacupuncture on Nociceptive Discharges of Spinal Wide Dynamic Range Neurons in Rat. J Pain Res. 2023;16:695–706. doi: 10.2147/JPR.S396481
3 Yu Q-Q, Sun X-Y, Chen J-K, et al. Distinct intensity of electroacupuncture ameliorates mechanical hypersensitivity by attenuating neuronal sensitization in spinal dorsal horn in a rat model of inflammatory muscle pain. J Integr Med. 2025;S2095-4964(25)00202-X. doi: 10.1016/j.joim.2025.12.010

You must be logged in to post a comment.