
Inspired by Zhao et al 2024.[1]
RCT – randomised controlled trial
PPT – pressure pain threshold
VAS – visual analogue scale
MCID – minimal clinically important difference– key to acronyms
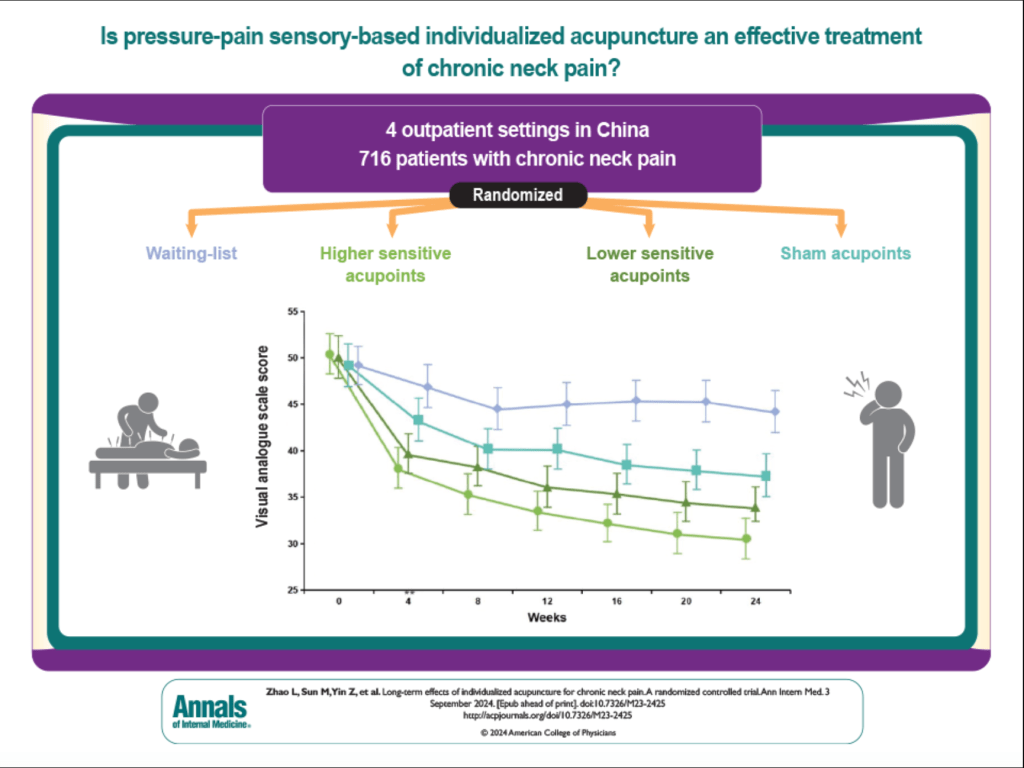
I reviewed this paper for Annals of Internal Medicine in September last year. It is a large 4 arm RCT (n=716) from a well-known group in Chengdu. This is the same group that brought us a paper in JAMA Internal Medicine that appeared to support point specificity in chronic stable angina: see Chronic stable angina and point specificity.[2]
The current paper has results that fit perfectly with physiological expectations, unlike the latter paper. The 4 arms were parallel and included 3 with acupuncture needling. The 4th arm was a waiting list control. One needling arm was designated sham, but needle insertion was of similar depth to the other groups (0.5 to 1.0cun). They did describe it as shallow acupuncture, no typical needling sensation (deqi) was sought, and the points were away from recognised acupuncture points, although 4 of the five points were on the arms and therefore segmental for chronic neck pain.
The true acupuncture groups targeted acupuncture points in the neck, shoulders, and upper limbs based on PPT measurements of a standard set of the 15 most commonly used acupuncture points for chronic neck pain. One group selected the 5 most sensitive points, and the second group selected the 5 least sensitive points. PPT was reassessed after 2 weeks of treatment.
10 sessions were applied over 4 weeks, 3 per week over the first 2 weeks and 2 per week for the following 2 weeks. The primary outcome was the change in VAS neck pain at 4 weeks from baseline.
The baseline VAS neck pain was ~50mm and there was a modest but clinically significant drop of just over 12mm and just over 10mm in the true acupuncture groups. The sham acupuncture group improved by just over 6mm and the waiting list group improved by just over 2mm.
Both acupuncture groups were significantly better than the sham or waiting list groups, which is not a particular surprise; however, the journal editors clearly insisted on making a statement about the clinical significance of the size of the mean group differences, which did not reach 10mm. I have argued many times about the application of MCIDs to differences in group means in RCTs. When estimated in prospective research, MCIDs are always measured from baseline and cannot be assessed by measuring differences in group means; therefore, applying these measures to the latter in subsequent RCTs makes no sense.
For acupuncturists who often select the more sensitive points in clinical practice, this research does not support that approach, despite a small trend in that direction.
I was curious to see which were the more sensitive and less sensitive points used, and shocked to see GB20 at the bottom of the sensitive point list. Top of the list was TE15. That got me thinking about the difference between clinical examination with fingertips and measurement of PPT with an algometer. At TE15 an algometer can fairly easily squeeze trapezius onto the upper medial edge of the scapula – this area is always tender, but that tenderness is artificial (generated by anatomy) rather than pathophysiological.
But what about GB20 – surely that is also a very commonly tender point? The tenderness at GB20 is most commonly elicited by a small cross-fibre palpation of semispinalis rather than a static pressure in one direction, as would be generated by the footplate of an algometer.
Perhaps this is one reason for the surprising lack of difference between treating sensitive and non-sensitive points in this trial.
References
1 Zhao L, Sun M, Yin Z, et al. Long-Term Effects of Individualized Acupuncture for Chronic Neck Pain : A Randomized Controlled Trial. Ann Intern Med. Published Online First: 3 September 2024. doi: 10.7326/M23-2425
2 Zhao L, Li D, Zheng H, et al. Acupuncture as Adjunctive Therapy for Chronic Stable Angina: A Randomized Clinical Trial. JAMA Intern Med. 2019;179:1388–97. doi: 10.1001/jamainternmed.2019.2407

You must be logged in to post a comment.