
Inspired by Shew et al 2019.[1]
This is the first reported case of a spinal epidural abscess as a possible complication of acupuncture treatment in New Zealand. It is the 15th such report I can find in the literature (on PubMed), but this report and most others cannot make irrefutable causal links between acupuncture needling and abscess formation, leaving us wondering between consequence and coincidence.
Acupuncture and epidural abscesses
epidural abscess AND acup* [abti]
Put this term in the search box of PubMed and you will find 17 citations, of which one is a case of endophthalmitis,[2] and one is not related to acupuncture, but acupuncture is mentioned in the abstract as a risk factor for the condition.[3]
The epidural fat layer is apparently a great place for growing bugs, but fortunately for humankind it is not easily accessible. Spread of infection to the space is usually via blood (about half of cases), but can also be via contiguous spread (about a third of cases).[4] I am referring to spinal epidural abscesses in general here, rather than simply those related to acupuncture. In the 15 cases I mentioned above,[1,5–18] acupuncture in some form had been performed prior to diagnosis of the epidural abscess, and usually at the level of the abscess. It is possible that some patients sought acupuncture treatment for symptoms related to an already developing abscess or related infection. One exception,[5] where there seems to be little doubt about causation was the subject of a previous blog. Another notable case involved E coli (a pathogen from the bowel) as the causative organism, and a 100mm needle insertion at the same level in the back 3 days prior to presentation.[8]
On the other hand, some cases seem highly unlikely to involve a causative link. In one such case a 13-year-old boy had been suffering from lumbar pain one month before having a single ‘pyonex’ insertion over the right paraspinal muscles.[9] In those days pyonex needles were tiny metal press needles, like tiny drawing pins. They were not sterile, but the potential for infection via inoculation would have been very small due to their size and shape. Local infection with such needles was recorded, but only rarely, and after they were left in place for days or weeks. 24 hours after receiving this treatment the boy developed severe lumbar pain and a fever. On admission he had a temperature of 38.2°C, ESR 107, CRP 210 and WCC 14.3. Blood cultures were negative. An isotope scan indicated asymmetrical uptake at the right L4/5 facet, and MRI demonstrated a moderately large epidural collection presumed to be an abscess.
No local infection is mentioned, and no bacterium was isolated. The boy was treated with IV antibiotics followed by a long course of oral antibiotics and recovered uneventfully.
It is very difficult to interpret this case. A boy of 13 probably had numerous scratches and scrapes that amounted to a greater potential for inoculation than a single pyonex needle, and 24 hours seems rather too quick to develop such a collection as was seen on imaging. It is possible that the boy’s symptoms were already worsening, and that was the reason for seeking acupuncture the day before he spiked a temperature.
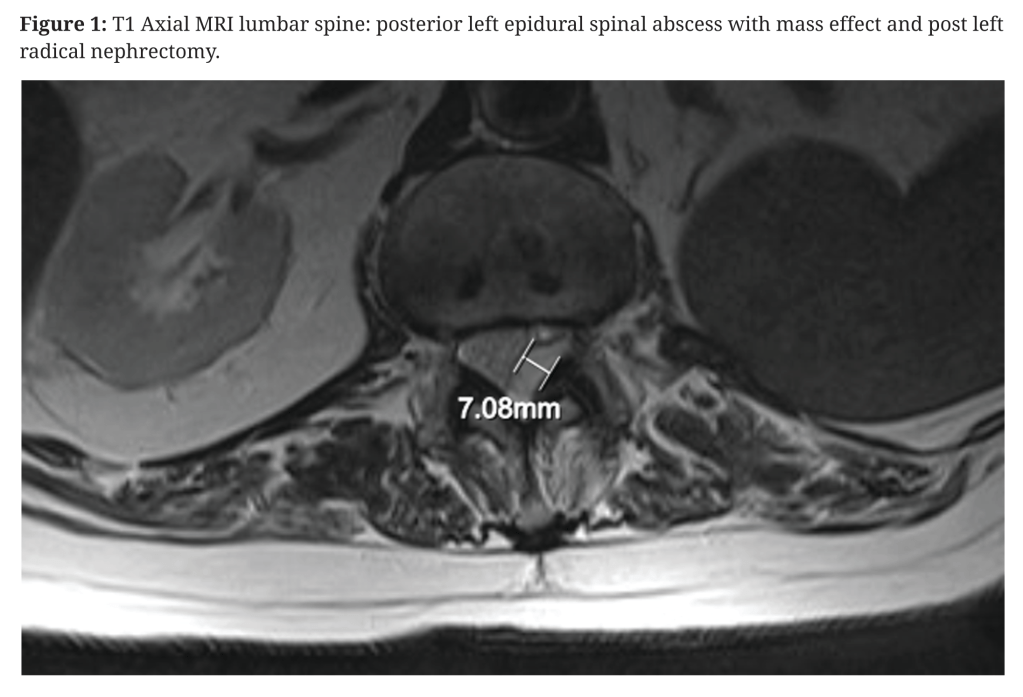
So, let’s have a look at this recent case.[1] An 89-year-old man with type 2 diabetes and diabetic nephropathy presented with a 2-week history of poorly characterised left flank and hip pain. He had undergone a left nephrectomy at some point in the past (not detailed) and attributed his pain to a fall some 3 months previously. He sought acupuncture for pain relief, but the timing is not reported. He was afebrile with raised CRP (122) and WCC (18.57). On day four of admission, he developed retention of urine and a subsequent MRI demonstrated a posterior left epidural abscess extending from T11 to L4/5.

The discussion starts with: “Inoculation of the infection-prone fat in the epidural space…”, and goes on to quote Darouiche’s estimates from NEJM that I mentioned at the start – about half of cases are via haematogenous spread and a third contiguous spread.[4] Inoculation implies the authors have assumed an acupuncture needle pushed Staph aureus from the skin into the epidural space, but this is very unlikely with a filifiorm needle since there is no bore to carry the bugs in, and most would be wiped off in superficial layers. In addition to this I doubt many acupuncture practitioners in New Zealand insert needles as far as the epidural space on a routine basis. In this case, based on the axial MR image in Figure 1 it would require a 50mm needle insertion close to the midline.
Let us suppose that acupuncture managed to push enough bugs under the skin and into the circulation to fascilitate haematogenous spread. In this case the location of needling is likely to be irrelevant, although it clearly is not to the authors who report the cases, as they invariably mention that the acupuncture needling was at the level of the abscess. I guess they all assume inoculation without consideration of the needle shape. Perhaps a needle placed down to the interspinous ligament, as is often done in classical acupuncture might have the possibility to cause a relatively superficial infection that can then spread contiguously along the edge of the ligament to the epidural space. Contiguous spread seems less likely from erector spinae because of the longitudinal distribution of muscle compartments. The patient was diabetic, thus increasing the risk of infection; however, only 4 of the 15 cases related to acupuncture involved diabetic patients.[1,10,14,17] This may be because most are coincidental associations rather than inoculations.
Having reviewed all 15 cases in detail, acupuncture seems clearly related in only a few, with many being described too poorly to judge, and in others it seems highly likely that the acupuncture was coincidental, or that the infection was already present. Indeed, I found one report that quoted the Hoffman paper on skin disinfection from Acupuncture in Medicine,[19] and concluded that the acupuncture was very unlikely to have been the causative agent.[13] Moreover, in a retrospective review of 128 cases from a specialist centre, acupuncture was not identified as a risk factor in any.[20] The most frequent risk factors were intravenous drug abuse (39.1%) and diabetes mellitus (21.9).
So, what can we learn? It doesn’t seem likely that we can prevent the very rare occurrences of infection by altering practice, provided we already adhere to the rule of clinically clean hands and puncture sites. The best we can do is to ensure the highest risk patients (diabetic, immunocompromised, frail elderly) with vague spinal symptoms see their usual doctor beforehand. With luck any occult infection can be picked up before our needles penetrate their skin and give the specialists who write up the subsequent case reports a target for blame and absolution from adequate consideration of the techniques, the timeline or alternative explanations.
Addendum
A senior colleague from Japan (Prof Hitoshi Yamashita) contacted me after reading this blog to let me know that the reference to a ‘pyonex’ in the Ishibe paper [9] was a mistranslation of ‘hari’ (needle) in a Japanese / English dictionary – he had contacted the author in the course of a safety review. So, in this case of the 13-year-old boy, a single acupuncture needle was used, not a press needle. This does not alter the analysis, but the clarification is very helpful and reassuring. The acupuncture specific details in these reports are always lacking.
On another note, it is very reassuring for me that my non-peer reviewed blogs get some post production review :-).
References
1 Shew W, Bell S. Unusual presentation of spinal epidural abscess and a cautionary tale of acupuncture. N Z Med J 2019;132:69–72.
2 Lee S-Y, Chee S-P. Group B Streptococcus endogenous endophthalmitis : case reports and review of the literature. Ophthalmology 2002;109:1879–86.
3 Pons M, Pérez L, Juárez F. [Pediatric case report: Spinal epidural abscess]. Arch Argent Pediatr 2017;115:e146–9. doi:10.5546/aap.2017.e146
4 Darouiche RO. Spinal epidural abscess. N Engl J Med 2006;355:2012–20. doi:10.1056/NEJMra055111
5 Priola SM, Moghaddamjou A, Ku JC, et al. Acupuncture induced cranial epidural abscess: Case report and review of the literature. World Neurosurg Published Online First: 8 February 2019. doi:10.1016/j.wneu.2019.01.189
6 Yu H-J, Lee K-E, Kang HS, et al. Teaching NeuroImages: multiple epidural abscesses after acupuncture. Neurology 2013;80:e169. doi:10.1212/WNL.0b013e31828c2f1d
7 Lee J-H, Cho J-H, Jo D-J. Cervical epidural abscess after cupping and acupuncture. Complement Ther Med 2012;20:228–31. doi:10.1016/j.ctim.2012.02.009
8 Bang MS, Lim SH. Paraplegia caused by spinal infection after acupuncture. Spinal Cord 2006;44:258–9. doi:10.1038/sj.sc.3101819
9 Ishibe M, Inoue M, Saitou K. Septic arthritis of a lumbar facet joint due to pyonex. Arch Orthop Trauma Surg 2001;121:90–2.
10 Yazawa S, Ohi T, Sugimoto S, et al. Cervical spinal epidural abscess following acupuncture: successful treatment with antibiotics. Intern Med 1998;37:161–5.
11 Alexandre AR, Raimundo P. Epidural, paravertebral and bilateral psoas abscess after lumbar acupuncture. BMJ Case Rep 2018;11:e228047. doi:10.1136/bcr-2018-228047
12 Ma F, Kang M, Liao YH, et al. Nocardial spinal epidural abscess with lumbar disc herniation: A case report and review of literature. Medicine (Baltimore) 2018;97:e13541. doi:10.1097/MD.0000000000013541
13 Cupler ZA, Anderson MT, Stancik TJ. Thoracic Spondylodiscitis Epidural Abscess in an Afebrile Navy Veteran: A Case Report. J Chiropr Med 2017;16:246–51. doi:10.1016/j.jcm.2017.03.002
14 Kim DM, Kim SW. Destruction of the C2 Body due to Cervical Actinomycosis: Connection between Spinal Epidural Abscess and Retropharyngeal Abscess. Korean J Spine 2017;14:20–2. doi:10.14245/kjs.2017.14.1.20
15 Chan JJ, Oh JJ. A rare case of multiple spinal epidural abscesses and cauda equina syndrome presenting to the emergency department following acupuncture. Int J Emerg Med 2016;9:22. doi:10.1186/s12245-016-0116-5
16 Godhania V. Lumbar spine osteomyelitis and epidural abscess formation secondary to acupuncture. J Surg case reports 2016;2016. doi:10.1093/jscr/rjw035
17 Yao Y, Hong W, Chen H, et al. Cervical spinal epidural abscess following acupuncture and wet-cupping therapy: A case report. Complement Ther Med 2016;24:108–10. doi:10.1016/j.ctim.2015.12.002
18 Yang C-W, Hsu S-N, Liu J-S, et al. Serratia marcescens spinal epidural abscess formation following acupuncture. Intern Med 2014;53:1665–8.
19 Hoffman P. Skin disinfection and acupuncture. Acupunct Med 2001;19:112–6.
20 Patel AR, Alton TB, Bransford RJ, et al. Spinal epidural abscesses: risk factors, medical versus surgical management, a retrospective review of 128 cases. Spine J 2014;14:326–30. doi:10.1016/j.spinee.2013.10.046

You must be logged in to post a comment.