
Stimulated by Tucciarone et al and Choi et al 2019.[1,2]

These two papers popped up on one of my PubMed searches on Monday 22nd July. They are both adverse events related to acupuncture in the region of the spine. One avoidable, and the other probably not, and both in relatively young and otherwise fit men.
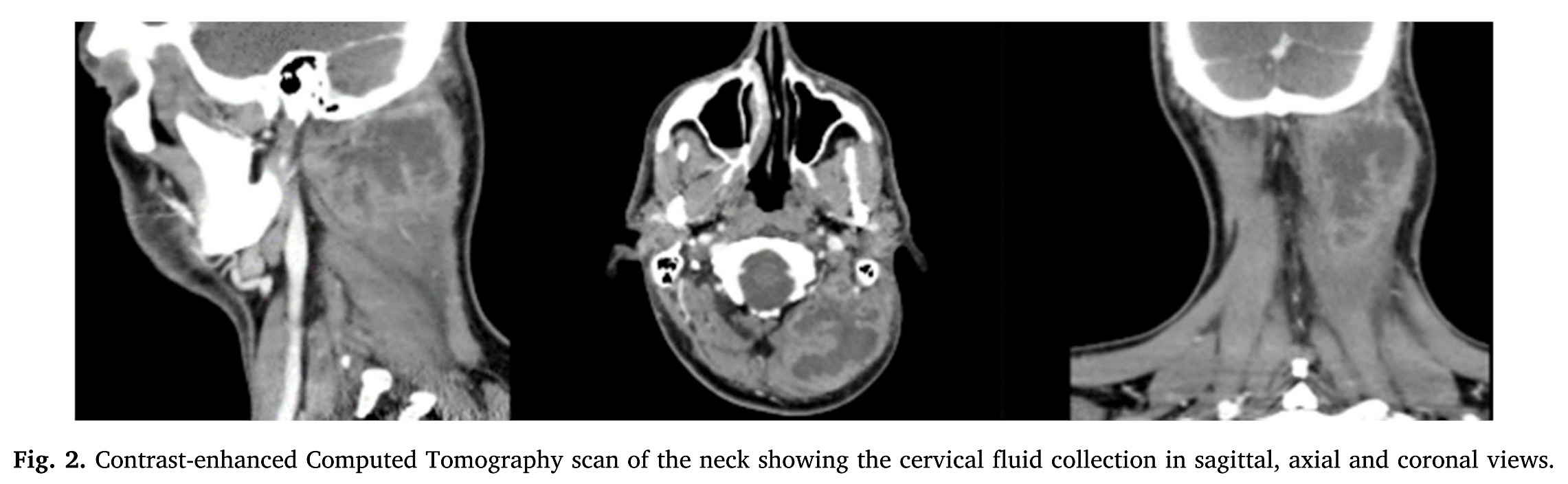
First is a rather rare case of muscle infection. The bug was a familiar one – Streptococcus pyogenes. This was potentially a simple inoculation of skin flora at what looks to be the region of GB20 in the neck. The patient, a 36-year-old man had 3 sessions of acupuncture for a stiff neck within the previous fortnight. The contrast enhanced CT images of his neck show a rather large soft tissue swelling with an extensive fluid collection within it. The patient was successfully treated with open surgical drainage and systemic antibiotics. It is not clear that he had any predisposition to such infection, and the bug appeared sensitive to standard antibiotics (amoxicillin and clavulanic acid). It is possible that the infection was present before the acupuncture treatment started of course. I should note that the case appears to have come from Madrid, but was published in a Turkish journal.
Such infections seem impossible to prevent, and acupuncture needles do not inoculate sufficient numbers of bugs to result in local infection of healthy tissue.[3] The number of cases where local infection requiring treatment resulted from acupuncture in the largest prospective survey to date was 27 out of 229 230 patients who were treated with an average of 10.2 sessions. In the same survey, systemic infection that needed treatment occurred in 3 cases. If we include these, then the rate of infection per treatment was roughly 1:80 000.
The second case is more instructive and interesting. It is a case set in Korea of a 27-year-old man who had acupuncture treatment for back pain. He had undergone a laminectomy for an L4/5 disc prolapse 7 years prior, and his back problem was referred to as a post laminectomy syndrome. Perhaps this indicates that he had a chronic problem and was prepared to do anything to treat it. A 10cm acupuncture needle was inserted into the centre of his back and angled laterally, presumably at or near the site of his pain, and therefore close to the site where the lamina was deficient following his previous surgery.
A 10cm acupuncture needle was inserted into the centre of his back and angled laterally…
Following the acupuncture, he developed a severe postural headache on standing or sitting up. His symptoms resolved after 5 minutes lying supine. After suffering this headache for 8 days he attended the pain clinic where the authors of the case report worked. They suspected a post dural puncture headache (PDPH), and proceeded to administer an interlaminar epidural blood patch (EBP) of moderately large volume (15ml) at the L2/3 level. This was not effective, so they investigated the presumed CSF leak. MR imaging did not show any abnormality, but MR myelogram indicated a diffuse CSF leak into the lumbar paraspinal muscles on the left. A further interlaminar EBP at L4/5 was also unsuccessful, so they proceeded to perform the rather less common transforaminal EBP at two levels – L3/4 and L4/5. Only 3ml of autologous blood was injected at each level with this approach – I guess because there is simply less space. The patient was symptom free the following morning. There is no comment on his original back pain, but I guess his mind had been on other things!
I found this case report interesting because I had not previously heard of a transforaminal EBP, and indeed there are currently only 5 citations on PubMed with this in the title, so I guess it is not so common.
The other critical aspect of this report is that we can surmise that the 10cm long Korean acupuncture needle probably passed through an iatrogenic defect in the lamina of L4 (from the previous laminectomy) and created a hole in the dural sheath surrounding the L4 nerve root. The interlaminar EBPs (with a total of 30mls of blood) did not reach far enough laterally to seal the hole or holes, but 3mls at the L4/5 foramen probably did.
…the 10cm long Korean acupuncture needle probably passed through a defect in the lamina of L4
We have discussed the potential risks of deep needling over the site of previous spinal surgery (where lamina may be deficient) for some 20 plus years on the BMAS Foundation Course, but this is the first case report where the details seem to suggest that such a risk is actually worth considering. There are similarities here to the first case of vertebral artery damage via direct needling of the back of the neck above C2. Another case from Korea.[4]
References
1 Tucciarone M, Taliente S, Gómez-Blasi Camacho R, et al. Extensive pyomyositis of prevertebral muscles after acupuncture: Case report. Turkish J Emerg Med 2019;19:113–4. doi:10.1016/j.tjem.2019.03.003
2 Choi YN, Kang SJ, Joo JD, et al. Targeted Transforaminal Epidural Blood Patch for Postdural Puncture Headache in Patients with Postlaminectomy Syndrome. Case Rep Neurol Med 2019;2019:1968314. doi:10.1155/2019/1968314
3 Hoffman P. Skin disinfection and acupuncture. Acupunct Med 2001;19:112–6.
4 Hong S, Park Y, Lee C-N. Lateral Medullary Infarction Caused by Oriental Acupuncture. Eur Neurol 2018;79:63. doi:10.1159/000479963

You must be logged in to post a comment.