Stimulated by Yuan et al 2019 and Sun et al 2020.[1,2]

I have added coloured dots over BL32, BL33 and BL35.
Rather similar to last week’s blog, I was drawn to the first of these papers by the comparison of techniques alluded to in the title: “Effect of depth of electroacupuncture…”
The second paper is a reanalysis of data from two large clinical trials, both of which have been highlighted on this blog in the past (EA for SUI and EA in MUI). The techniques used are rather similar to that used in this new trial by Yuan et al on BPH (Benigh Prostatic Hyperplasia), and of course there is great anatomical proximity of the conditions treated.
Yuan et al is a rather small study (n=60), but it shows some differences between performing electroacupuncture at different depths. The points used were BL32 and BL33. These lie directly over the second and third sacral foramina. The deep insertion group used 75mm needles, inserted to a depth of 60–75mm. The aim was to achieve sensation in the anterior pudendal area. I infer from this that the anatomical target was in the vicinity of the ventral sacral roots of S2 and S3 (the pudendal nerve derives from the ventral roots of S2–S4).
“a bellows effect visible at the perineum”
Dave
It is somewhat of a coincidence that I had a rather in-depth discussion of this anatomical area with a gastroenterologist colleague (Dave) in the teaching clinic yesterday. He implants leads for neuromodulation through the S3 foramina, and happily comments that they do not really know how it works. The similarity to a rather ancient form of neuromodulation is intriguing. I am pleased to report that Dave and I intend to continue our debate about what is happening, and which nerves are involved later in the year when I hope to join him in theatre to watch the process of lead positioning and testing. In an anaesthetised patient they rely on motor fibre stimulation to determine the correct position. If the ipsilateral big toe flexes, that is S2, but if the toes flare out and there is a bellows effect visible at the perineum then that is S3 – the target nerve.
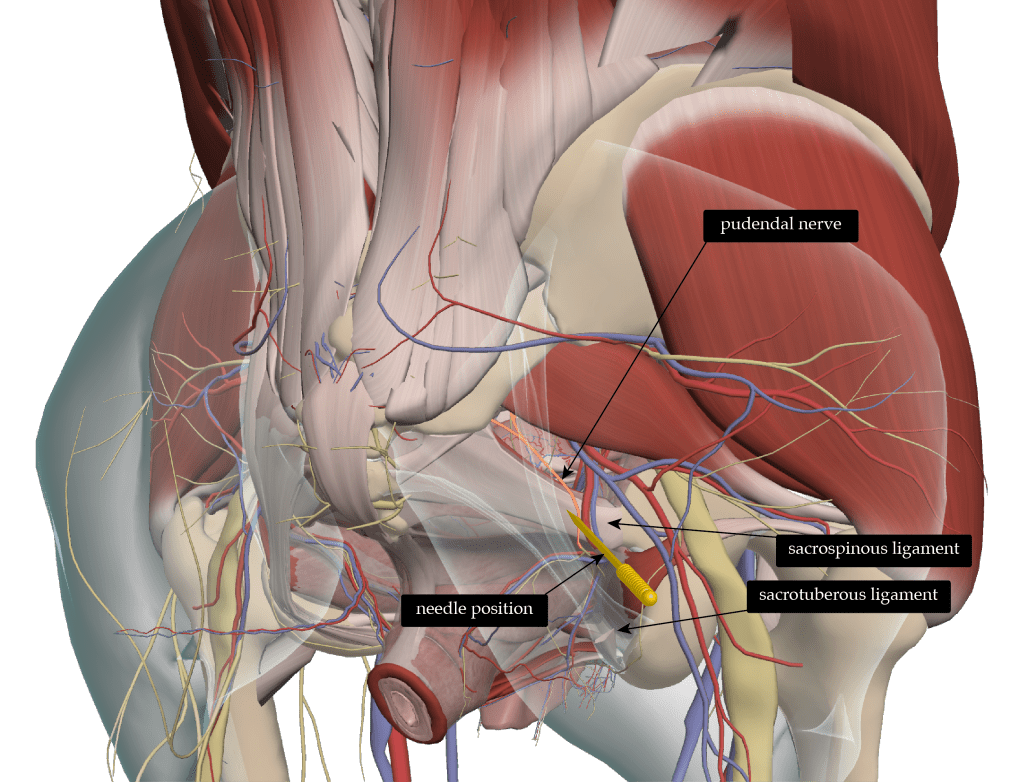
This reminds me of a discussion I had in Porto Alegre with the lovely Vera a few years ago – she was appointed as my translator. Vera was known locally as ‘the pudendal queen’, presumably for her adeptness at being able to target the nerve of the same name as it tracks along the top of the sacrospinous ligament. We were discussing the sensory effects of direct pudendal nerve stimulation, because this is what they use to determine the correct needle placement. Vera told me that one of her more elderly patients commented that they ‘had not felt anything quite like that for a very long time’ when referring to the sensation felt in the pelvic floor.
We have published a discussion of how to target the nerve in the journal, and the pros and cons of different approaches in Acupuncture in Medicine.[3]
So back to Yuan et al, and their needles in the sacral foramina compared with more superficially. I should note at this point that their idea of more superficial sounds rather like what I do routinely, and I am not accustomed to being referred to as superficial – at least not in respect of my needling style! The superficial insertion of Yuan et al used 40mm needles and inserted them 25-40mm and manipulated them to generate needling sensation. Ok, I guess I do go a little deeper than this, it all depends on the depth of the subcutaneous fat and thickness of multifidus. I aim to touch the sacrum at S2 and S3, which could be anything from 40 to 60mm or more.
The deeper insertions into foramina, along with 20Hz EA for 30 minutes, 12 times in 4 weeks was associated with a significantly improved outcome on the IPSS compared with the superficial insertion EA group. The IPSS is the International Prostate Symptom Score, and the total score improved significantly in both groups, but was improved most in the deep insertion group. Quality of life improved in both groups with greater improvement in the deep insertion group. The more objective outcomes did not follow the same pattern. Post void residual urine reduced significantly in both groups, being numerically but not significantly better in the superficial group. Qmax (maximum urinary flow rate) improved numerically in both groups to a small degree, but this was not a significant pre-post change. I guess that is not a big surprise since we would not expect the physical size of the prostate to alter, and indeed it is comforting to see this reported as a negative outcome, since it gives us more confidence in the veracity of the other data (in a journal that may not have the same level of rigour that we like to apply in Acupuncture in Medicine – 😉 no bias there then).
Sacral EA for stress urinary incontinence (SUI)
The second paper I am highlighting examined the effect of sacral EA on SUI (stress urinary incontinence) in elderly women. It took the data from two previous trials, selected those patients with SUI or stress predominant MUI (mixed urinary incontinence), and compared the outcomes in elderly and non-elderly women. Out of a total of 1004 women in the two trials, 384 received EA for SUI, and this group was divided by age – elderly was defined by WHO criteria as >60 years. The main outcome was the proportion of women with a 50% or greater improvement (reduction) in 72-hour IEF (Incontinence Episode Frequency). Perhaps it is no big news that there was no difference between the groups in terms of outcomes, but it should be noted that the groups differed significantly at baseline in several respects. Of course, they differed by age, and not surprisingly by the percentage in the menopause, but also by duration and severity of SUI. So in brief this was a more severely affected cohort, and one that takes longer to recover from surgical treatments for SUI, and for whom surgical treatments may be less effective.
The EA treatment in these trials was a little different from that described above. They used deep insertion at BL33, so needles placed into the S3 foramina, together with deep insertion in a superolateral angulation at BL35 (just lateral to the coccyx).
The key structure to avoid here is the rectum, and needles placed into the S4 foramina have been measured at an average of 6mm away from the rectum.[4]
My preference will be to use S2 and S3…
Well on the whole this is a positive story, and I am tempted to skill up and start using this deep insertion protocol. My preference will be to use S2 and S3, since we have published in Acupuncture in Medicine a CT study demonstrating a theoretically greater safety profile of this approach.[4]
Before I sign off this week, and still on the subject of deep needling in the sacral region, I was shocked to see a paper this morning describing long needle insertion from BL54 (just lateral to the sacrum at S4) to ST28 (mid rectus abdominis 50mm above the pubis). This was part of a treatment protocol advocated for dysmenorrhoea. They describe inserting needles 100 to 150mm from BL54. Well this is not long enough to reach the rectus abdominis, which would be roughly 300mm, but it would be deep enough to penetrate bowel. Indeed, the authors include an image of a male cadaver with a skewer inserted halfway from the back to the front. The slice is in a sagittal plane through the left pubic bone and sacroiliac joint, and the skewer is placed just below the large iliac vessels and in the direction of a section of the large bowel. Not only is this a male cadaver, but the image was taken in 1997, so I guess that it was not produced especially for this paper.
31 women received this treatment, and there were no complications, but I am still alarmed that this sort of technique is advocated without sufficient justification. Nerves to viscera do not respond to needle insertion so there is no advantage to needle placement in this location, and whilst acupuncture needles are unlikely to penetrate healthy bowel, why on earth take the risk? We certainly know from case reports of adverse events that bowel penetration with subsequent infection has been reported many times (see Retroperitoneal abscess with pylephlebitis on the blog under Adverse events).
References
1 Yuan H, Wei N, Li Y, et al. Effect of Depth of Electroacupuncture on the IPSS of Patients with Benign Prostatic Hyperplasia. Evidence-Based Complement Altern Med 2019;2019:1–7. doi:10.1155/2019/1439141
2 Sun B, Liu Y, Su T, et al. Electroacupuncture for stress-related urinary incontinence in elderly women: data analysis from two randomised controlled studies. BMJ Support Palliat Care 2020;0:1–7. doi:10.1136/bmjspcare-2019-002034
3 Oliveira e Lemos M, Cummings M. An Alternative Approach to Pudendal Nerve Stimulation. Acupunct Med 2018;36:423–4. doi:10.1136/acupmed-2018-011751
4 Katayama Y, Kamibeppu T, Nishii R, et al. Ct Evaluation of Acupuncture Needles Inserted into Sacral Foramina. Acupunct Med 2016;34:20–6. doi:10.1136/acupmed-2015-010775

You must be logged in to post a comment.