
Stimulated by Chen et al 2021,[1] and Narayana Murthy et al 2021.[2]
TKA – total knee arthroplasty
key to acronyms
IF – impact factor
RCT – randomised controlled trial
This week I have chosen a couple of papers that are linked by virtue of the patients having metalwork in one or both knees. The first paper is a systematic review studying the effect of acupuncture on rehabilitation after total knee arthroplasty (TKA), and the second is a rare adverse event that serves as a warning for practitioners treating patients with TKA or indeed any implanted metalwork that is relatively close to the skin surface.
part of the largest urban agglomeration on the planet
The review group comes from two centres in China: Guangzhou, which is just above Macau and part of the largest urban agglomeration on the planet; and Kunming, the capital of Yunnan province, which is in the far southwest of China.
The review is published in Frontiers in Medicine (IF 3.00), and includes 9 RCTs: 4 from mainland China, and one each from Taiwan, Hongkong, Japan, Denmark and Spain. There was clearly quite a bit of clinical heterogeneity in that the treatments varied from a single session to 10 sessions over 2 weeks. There was also a range of different outcome measures and time points for evaluation, meaning that data from only 2 or 3 trials could be pooled in meta-analysis for most outcomes.
The results demonstrated a fairly convincing effect on pain from 8 to 48 hours after surgery, but no longer-term effect, and no obvious effect on function. The latter outcomes were considerably hindered by statistical heterogeneity, but when you go and look at the details of the individual trials you realise that the clinical heterogeneity is astonishing. It makes me wonder why some methodologist hasn’t written a guideline on what you should and should not pool. Then I realise that a methodologist might not fully appreciate the degree of clinical heterogeneity without having some clinical experience in the relevant field, and that reminds me of a drive to exclude clinicians from systematic reviews because they are too biased! So, we end up with the blind leading the blind… great for excluding bias, but not great for making common sense decisions over pooling data.
the widest diamond I have ever seen
My favourite forest plot from this review is a day 21 or >21 pain outcome that pools data from two trials (from Japan and Spain), and has the widest diamond (the symbol at the bottom of the plot representing the pooled data) I have ever seen in such a plot. It caused me to check the details of the trials, and the differences between them. Well actually, it would be quicker to list the similarities… there was only one: that the patients all had TKR. One trial used a single dry needling session pre-op, and the other applied 3 sessions of acupuncture per week for 2 weeks from 7 days post op. The outcome was taken from immediately after the 6 sessions in one trial and combined with an outcome taken 4 weeks after the single treatment in the other. One trial used dry needling compared with sham and the other applied a course of acupuncture in addition to basic rehabilitation compared with basic rehabilitation alone. It is perhaps no surprise that there was considerable heterogeneity when the results of these were pooled.
The review is nicely laid out, with the key information from each of the included papers, including the points used. I was pleased to see that points directly over the knee joint were only used in one of the 9 RCTs, which brings me onto the second paper I want to highlight.
Granulicatella adiacens
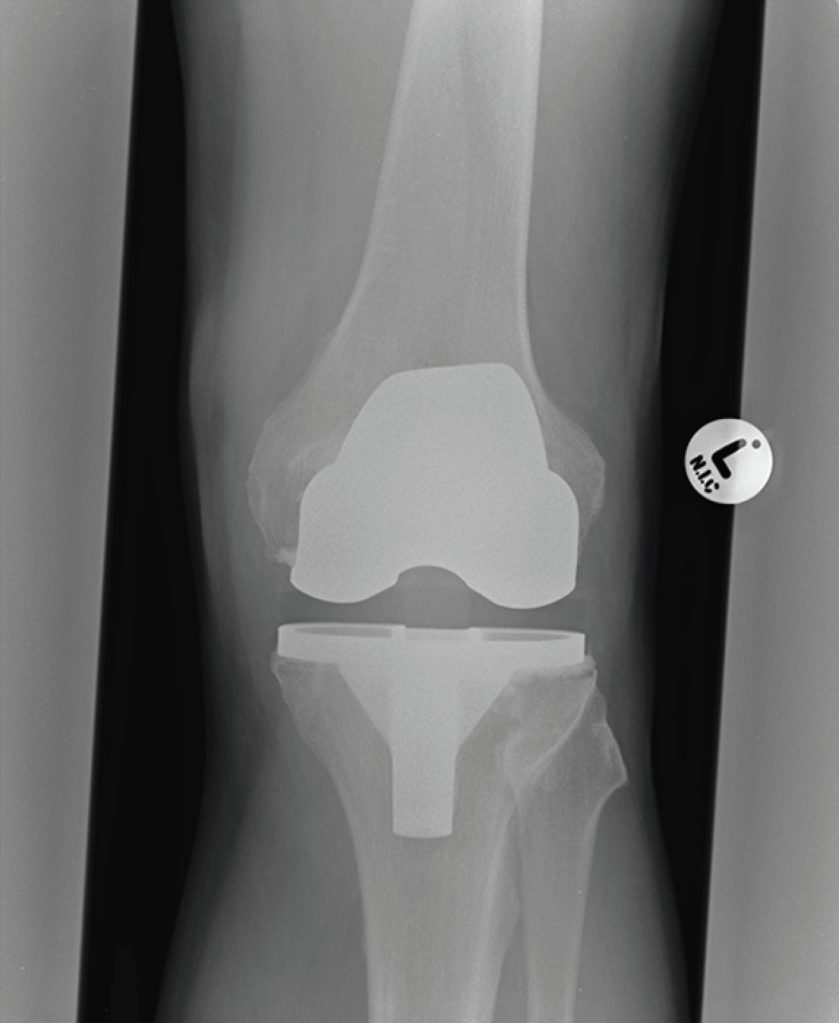
This is a case report of an infection in a prosthetic knee joint following acupuncture. A 65-year-old man who had undergone TKR for osteoarthritis 2 years previously received acupuncture treatment for hay fever that included insertion of a needle on the medial aspect of his knee. Three days later he attended the emergency department with a swollen painful knee. I am assuming it was the left knee from the x ray film with a big ‘L’ on it, but the report is a little slim on that sort of detail. Instead we have lots of details of blood tests, antibiotics and, of course, the rather rare bug responsible for the infection – Granulicatella adiacens.
Judging by the soft tissue shadow on the x ray film the prosthesis was between about 10 to 20mm beneath the surface on both medial and lateral aspects of the knee, so inoculation with an acupuncture needle is certainly possible. Spontaneous infection via a haematogenous route is also possible, but this would be a rather less likely coincidence at day 3 following needle insertion at the same site.
This is only the second reported case of infection of an orthopaedic implant in the knee,[2,3] but perhaps the eighth report of joint infection following acupuncture.[2–9] Whilst there may be under reporting, it is probably a rare complication of acupuncture; however, septic arthritis can have such devastating consequences that we should do our best to avoid it at all costs. For me that means never needling into joint spaces or onto the surface of a prosthesis.
References
1 Chen Z, Shen Z, Ye X, et al. Acupuncture for Rehabilitation After Total Knee Arthroplasty: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Front Med 2021;7:602564. doi:10.3389/fmed.2020.602564
2 Narayana Murthy S, Srinivasan SH, Maheswaran A, et al. Prosthetic knee joint infection by an unusual organism following acupuncture treatment. Acupunct Med Published Online First: 7 February 2021. doi:10.1177/0964528421990661
3 Laing AJ, Mullett H, Gilmore MFX. Acupuncture-associated arthritis in a joint with an orthopaedic implant. J Infect 2002;44:43–4. doi:10.1053/jinf.2001.0911
4 Woo PCY, Lau SKP, Yuen K-Y. First report of methicillin-resistant Staphylococcus aureus septic arthritis complicating acupuncture: simple procedure resulting in most devastating outcome. Diagn Microbiol Infect Dis 2009;63:92–5. doi:10.1016/j.diagmicrobio.2008.08.023
5 Tien C-H, Huang G-S, Chang C-C, et al. Acupuncture-associated Listeria monocytogenes arthritis in a patient with rheumatoid arthritis. Joint Bone Spine 2008;75:502–3. doi:10.1016/j.jbspin.2007.08.010
6 Daivajna S, Jones A, O’Malley M, et al. Unilateral Septic Arthritis of a Lumbar Facet Joint Secondary to Acupuncture Treatment – a Case Report. Acupunct Med 2004;22:152–5. doi:10.1136/aim.22.3.152
7 Ishibe M, Inoue M, Saitou K. Septic arthritis of a lumbar facet joint due to pyonex. Arch Orthop Trauma Surg 2001;121:90–2.
8 Lau S-M, Chou C-T, Huang C-M. Unilateral sacroiliitis as an unusual complication of acupuncture. Clin Rheumatol 1998;17:357–8. doi:10.1007/BF01451023
9 Kirschenbaum AE, Rizzo C. Glenohumeral pyarthrosis following acupuncture treatment. Orthopedics 1997;20:1184–6.

You must be logged in to post a comment.