
Inspired by Li et al 2022.[1]
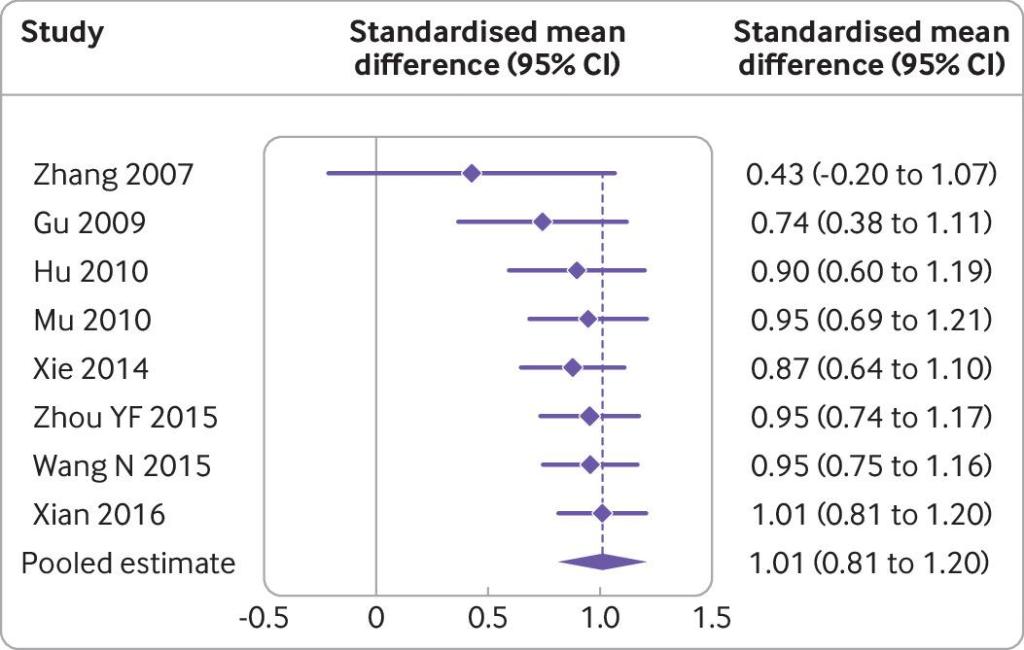
Cumulative meta-analysis of the use of acupuncture compared with language rehabilitation for functional communication in patients with post-stroke aphasia. Note that the values of each row are pooled estimates of all the previous trials plus the named trial of that row.
PSA – Post-Stroke Aphasia
key to acronyms
PSA – Prostatic Specific Antigen (not the subject of this blog)
GRADE – Grading of Recommendations, Assessment, Development and Evaluation (a method of grading the quality or ‘certainty’ and strength or ‘effect size’ of evidence in healthcare)
SR – systematic review
IF – impact factor
RCT – randomised controlled trial
CNS – central nervous system
MA – manual acupuncture
EA – electroacupuncture
SMD – standardised mean difference
I chose this paper to have a look at because the condition (post-stroke aphasia) had come up in the recent BMJ series of papers on acupuncture research as one where there was ‘good’ evidence of effectiveness, but no recommendations in guidelines.[2] Good here means a moderate or large effect size (in meta-analysis) with moderate or high certainty (in the GRADE assessment).
I have never been in a position to try treating this condition, and since it was highlighted at the top of the list of overlooked conditions (in terms of evidence) I thought I better not ignore it.
The recent paper I am highlighting is an SR summarising the acupuncture methods, neuroimaging techniques and possible cerebral mechanisms of PSA recovery with acupuncture. The paper is published in an open access journal called Neural Plasticity (IF 3.599), which has been around since 1989 under a couple of different names: the Journal of Neural Transplantation from 1989 to 1991 and the Journal of Neural Transplantation and Plasticity from 1991 to 1997. It dropped the neural transplantation and became the more succinct Neural Plasticity in 1998 – probably very sensible since the former phrase conjures up the horror fiction genre in my mind.
Tongue acupuncture
They included 16 studies, of which 8 were RCTs and 8 were observational studies. Perhaps I should not have been surprised to see that points in the tongue were used in a third of the studies. These points target the veins on either side of the frenulum on the underside of the tongue, and they each have their own unique name – Yuye on the left and Jinjin on the right. My impression is that they are pricked briefly to cause bleeding and the technique may have originally developed in an attempt to prevent asphyxiation from tongue swelling. Anyway, PSA is more of a CNS problem than a tongue problem, so I will not be rushing to needle any PSA patients I encounter in the vicinity of both of their lingual arteries, particularly after hearing what can go wrong with tongue piercings.
…but MC prefers CV23
I much prefer to use the other point that was chosen with a similar frequency to the tongue points – CV23, which is just above the hyoid bone and therefore also technically into the tongue, or at least muscles in the base of the tongue. It is inserted towards GV20 (at the vertex of the skull) and may just reach the genioglossus muscle – a muscle which is the most different in humans relative to other mammals apparently.[3] There are quite a lot of citations in PubMed with genioglossus in the title, which reflect its importance in opening, or not, the airway behind the tongue, and therefore its relevance in obstructive sleep apnoea.
I first got interested in the point CV23 when it was used with some success in this condition in a study from Brazil.[4] Interestingly, in this small 4-armed study (n=40), MA and 10Hz EA had a significant immediate effect on sleep apnoea and 2Hz EA did not. A previous trial by the same team (n=36) had already demonstrated an effect of a course of 10 sessions of MA over sham and a no treatment control.[5] I met the lead author of these studies, Anaflávia Freire, on my first trip to Brazil in 2009, where I first heard about this research.
Getting back to PSA, I tracked down the SR mentioned in the BMJ paper,[6] because the Forest plot in the BMJ paper (see above) looked a bit odd at first to me. Sure enough there were inconsistencies in some of the data represented, so I contacted Madison (the coordinating lead author of the recent BMJ series) and she explained the way the cumulative meta-analysis had been represented. The pooled estimate was correct, but each line above with an author and a date was sequentially pooled data rather than the unique data for each trial. I had not seen this before, but it makes sense now thanks to Madison’s rapid response on a Sunday morning.
Large effect size (SMD 1.01) for adding acupuncture to language rehabilitation in PSA
The effect size (SMD) for adding acupuncture to language rehabilitation was over 1 (0.8 or above is said to be a large effect). This came from 8 RCTs with 481 patients. The treatment schedule was typically around 4 weeks with 3 to 6 treatments a week, so this would be impossible to do in the West without significant infrastructure development, especially considering that around 38% of stroke patients suffer from aphasia.
As a methodological aside, and because acupuncture evidence often gets downgraded due to ‘unexplained’ heterogeneity, I was interested to note Zhang et al’s use of funnel plots to tease out the effect of using different outcome measures… I’ll have to show you at the webinar on Wednesday!
The neuroimaging findings of the SR are naturally rather preliminary and speculative. They focus on activation of Broca’s area and Wernicke’s area, and their functional connectivity with related areas, but there is a lot more to be done to make sense of what acupuncture might be doing in PSA aside from tickling veins on patients’ tongues.
Addendum
As of Wednesday morning on the 11th May 2022, I see a new SR on my PubMed searches on PSA from the same team as published the highlighted paper.[7] It has a couple of more recent RCTs in it than were included in the SR from 2019 and the BMJ paper.
The result is still positive but the results of the more recent trials are not as positive as the previous pooled value, and the conclusions of these review authors are somewhat more cautious than those of the BMJ paper.
References
1 Li B, Deng S, Sang B, et al. Revealing the Neuroimaging Mechanism of Acupuncture for Poststroke Aphasia: A Systematic Review. Neural Plast 2022;2022:5635596. doi:10.1155/2022/5635596
2 Lu L, Zhang Y, Tang X, et al. Evidence on acupuncture therapies is underused in clinical practice and health policy. BMJ 2022;376:e067475. doi:10.1136/bmj-2021-067475
3 Sanders I, Mu L. A three-dimensional atlas of human tongue muscles. Anat Rec 2013;296:1102–14. doi:10.1002/ar.22711
4 Freire AO, Sugai GCM, Togeiro SM, et al. Immediate effect of acupuncture on the sleep pattern of patients with obstructive sleep apnoea. Acupunct Med 2010;28:115–9. doi:10.1136/aim.2009.001867
5 Freire AO, Sugai GCM, Chrispin FS, et al. Treatment of moderate obstructive sleep apnea syndrome with acupuncture: a randomised, placebo-controlled pilot trial. Sleep Med 2007;8:43–50. doi:10.1016/j.sleep.2006.04.009
6 Zhang B, Han Y, Huang X, et al. Acupuncture is effective in improving functional communication in post-stroke aphasia : A systematic review and meta-analysis of randomized controlled trials. Wien Klin Wochenschr 2019;131:221–32. doi:10.1007/s00508-019-1478-5
7 Sang B, Deng S, Zhai J, et al. Does acupuncture therapy improve language function of patients with aphasia following ischemic stroke? A systematic review and meta-analysis. NeuroRehabilitation Published Online First: 29 April 2022. doi:10.3233/NRE-220007

You must be logged in to post a comment.