
Inspired by Chen C et al 2023 and Chen H-T et al 2023.[1,2]
Acup* – Acupressure or Acupuncture
key to acronyms
ARC – acute renal colic
RCT – randomised controlled trial
IV – intravenous
NSAID – non-steroidal anti-inflammatory drug
BCE – before common era (secular version of BC)
CE – common era (secular version of AD)
ICLpT – iliocostalis lumborum pars thoracis
L1 – the first lumbar vertebra
RR – response rate
AEs – adverse events
RoB – risk of bias
Acup* is the term I use when searching for papers on PubMed. The asterisk is called a ‘wildcard’ and it stands for any set of characters coming after the stem you type in before it. Until recent years, this term only selected the words ‘acupuncture’ and ‘acupressure’, so it was a very convenient way to narrow down on the relevant literature. Acupotomy, a form of acupuncture using chisel-like needles, is now a third possible result, but there are not so many papers on this particular technique – see my previous related blogs: Sciatica 2020 and Round acupuncture 2020.
I am using the term here to highlight two papers on treatment of ARC. One is an prospective cohort trial of acupressure versus IV parecoxib and the other is an SR of acupuncture versus a variety of different analgesic drugs.
This is the third year running I have a blog on ARC – clearly it has become popular in the 2020’s: Acupuncture for ARC 2021; Acupuncture for ARC 2022.
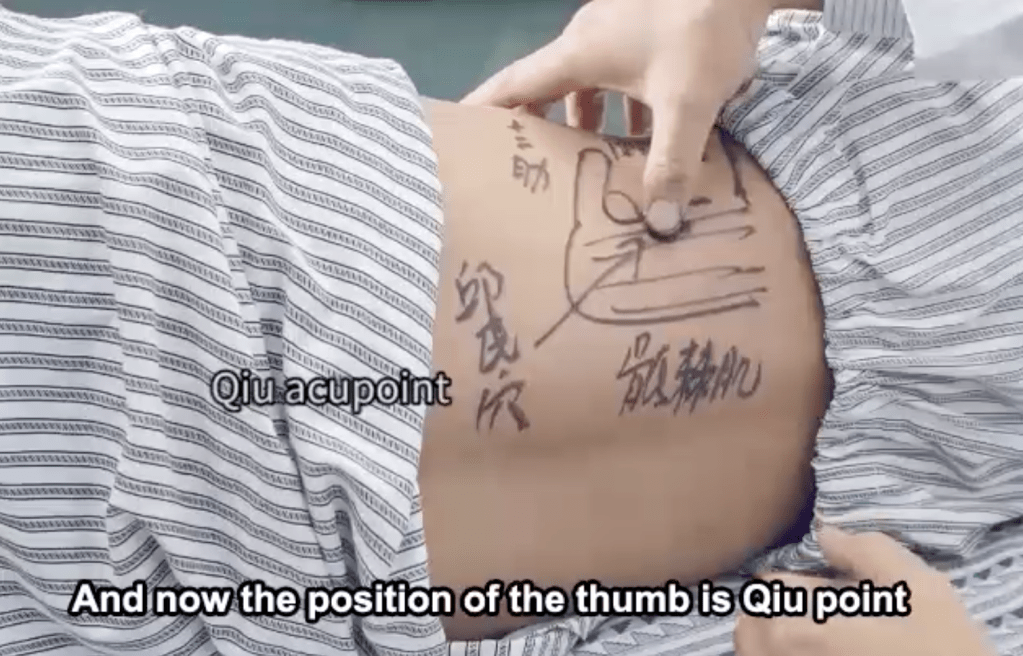
The first paper is a prospective cohort trial from Guangzhou (n=90). It is a straightforward comparative cohort trial of acupressure at a single point on the symptomatic side (called Qiu) against an IV injection of parecoxib (a selective NSAID). This point is not listed in any of my acupuncture textbooks or online (TCM Wiki). The point was described by one of the senior authors on the paper (Yunqiao Qiu), a urologist with decades of experience in treating ARC. So, it is relatively very contemporary in comparison with the classical acupuncture points, which date to the Han dynasty (206 BCE to 220 CE).
There is a nice video included as a supplemental file demonstrating how to find the point with a patient in the side lying position. Essentially, it is 2 thumb widths below the 12th rib in the outer erector spinae. Application of pressure at 45 degrees towards the midline with a thumb on this point would squeeze the lateral fibres of erector spinae muscles (principally ICLpT) onto the tip of the transverse process of L1. As this is a common site for trigger points in ICLpT, it is also likely to be a particularly sensitive point to pressure, notwithstanding the addition of a projection of a process of bone directly beneath.
According to the paper, this point was pressed by a single thumb on the painful side when the patient was side lying (painful side uppermost). The pressure was gradually increased for 1 minute. There is no mention of repeated application of acupressure.
The results of the trial are similar to those previously discussed with acupuncture techniques in the legs,[3] or hands,[4] as previously discussed on this blog. That is, a similar effect to the drugs at 30 minutes, but a much more rapid onset, such that pain reduced to an acceptable level within 5 minutes as opposed to just over 20 with the drugs.
The authors went on to perform propensity score matching of the groups to adjust for potential confounding factors, such as age, sex, left or right side, location, and size of stone. There was no difference in the results of the VAS pain scores. They went on to perform linear regression to compare the rate of decrease in VAS pain in the first 10 minutes between the groups and the effect of these potential confounders (called covariates in this analysis). Group allocation to acupressure ws the only variable that influenced the rate of decrease in VAS pain.
The second paper is a meta-analysis of RCTs of acupuncture versus a variety of drugs and drug combinations in the management of ARC. It included a total of 13 RCTs and 1212 patients. Acupuncture was slightly (~12%) better than the drugs in terms of response rate (RR) when all 13 trials were pooled. RR was determined by what each trial individually determined was the required reduction in pain to be considered a successful treatment.
Ten trials had data to pool on time to adequate pain relief. Acupuncture, as you might now expect, was faster by around 10 minutes. Five trials had data on pain scores between 30 and 60 minutes. Acupuncture was associated with marginally lower scores in this outcome. A meta-analysis of 4 trials and 314 patients assessed the risk of AEs. The risk of AEs with acupuncture was almost one tenth of that with the drugs.
Whilst this meta-analysis seems pretty convincing, we must acknowledge that RCTs directly comparing acupuncture with drugs are likely to be unblinded, with the exception of the double dummy methodology used in the most recent.[3] Where the outcomes are subjective (eg self-reported pain scores) this poses a high risk of bias, yet the RoB summary in this paper contains no red dots.
References
1 Chen C, Zhang Z, Lin M, et al. Acupressure versus parecoxib sodium in acute renal colic: A prospective cohort study. Front Med 2022;9:968433. doi:10.3389/fmed.2022.968433
2 Chen H-T, Kuo C-F, Hsu C-C, et al. Clinical efficacy of acupuncture for pain relief from renal colic: A meta-analysis and trial sequence analysis. Front Med 2022;9:1100014. doi:10.3389/fmed.2022.1100014
3 Zhang X, Liu X, Ye Q, et al. Acupuncture versus Lornoxicam in the Treatment of Acute Renal Colic: A Randomized Controlled Trial. J Pain Res 2021;14:3637–48. doi:10.2147/JPR.S339006
4 Tu J-F, Cao Y, Wang L-Q, et al. Effect of Adjunctive Acupuncture on Pain Relief Among Emergency Department Patients With Acute Renal Colic Due to Urolithiasis: A Randomized Clinical Trial. JAMA Netw Open 2022;5:e2225735. doi:10.1001/jamanetworkopen.2022.25735

You must be logged in to post a comment.