
Inspired by Dietzel et al 2019.[1]
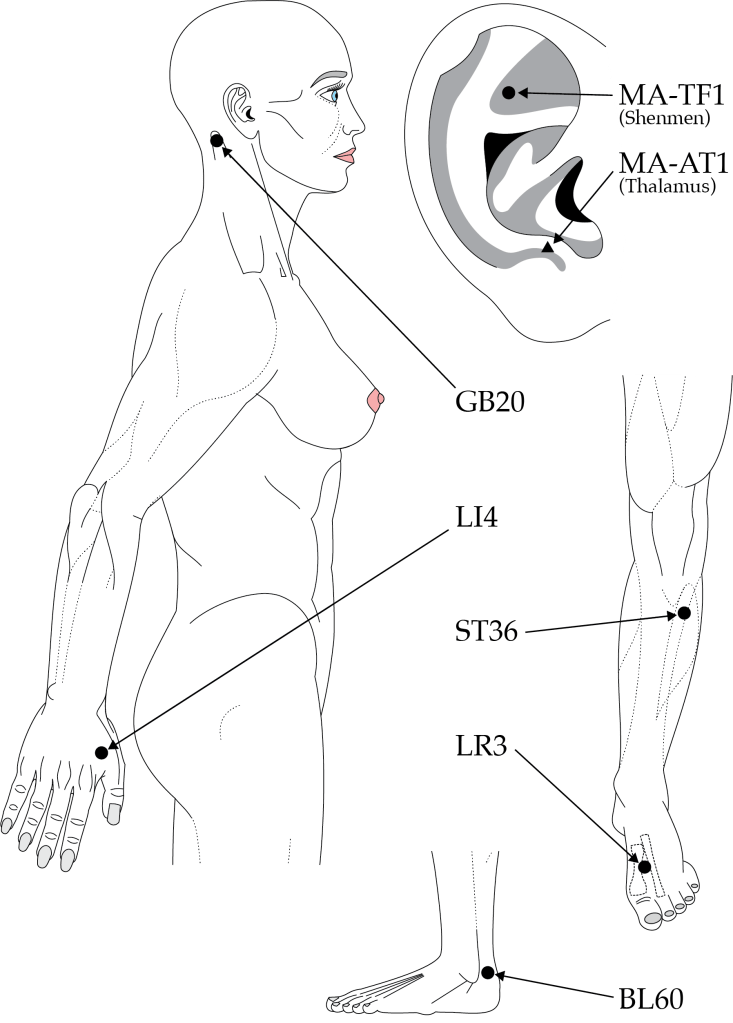
This paper was published very recently in the journal Neurocritical Care. I was more familiar with it than you might expect because, on request of the senior author, I had checked the English a couple of times for submissions to different journals and I had created the diagram illustrating point locations.
As an aside, it is always entertaining to see my rather muscular female body diagrams in official publications, with their bright blue eyes, long eyelashes and fingernails. Not to mention the pink lips and nipples of course…
I did the diagrams for a textbook some years ago and handed over the ai files to the publisher’s graphic designers because they were “not to their usual standards”. When I saw the proofs, I noted that the only changes were the removal of the eyelashes, and the colour. To my amusement they had overlooked the long nails on the females.
They had also taken the frown lines off the male, so to my eyes it looked as though I had had Botox.
it looked as though I had had Botox 😀
But I digress, this is supposed to be a research review!
Subarachnoid haemorrhage (SAH) is classically associated with sudden onset of severe headache, ‘as if hit over the back of the head with a baseball bat’. I often use this example in WMA courses of the type of headache to avoid treating with acupuncture. The context is that we are training healthcare professionals to use acupuncture as a therapy and headache is a common indication. But the critical step is the decision to treat, and consideration of the individual’s scope of practice. All professionals attending our courses and competent to treat headache, but most are not competent to assess patients with recent onset severe headache and decide whether or not acupuncture treatment is appropriate.
acupuncture was successful in treating drug resistant headache due to cerebral vasospasm associated with aneurysmal SAH
So it is somewhat ironic that I highlight this paper. It is a report of three cases in which acupuncture was successful in treating drug resistant headache due to the cerebral vasospasm associated with aneurysmal SAH (aSAH). The key aspect is that the acupuncture was provided in hospital and after diagnosis and definitive treatment of the bleeding aneurysms, not beforehand. In all three patients the headache intensity was rated as 10 out of 10 before acupuncture, and after 3 daily sessions it was 0, 1 or 2 out of 10 respectively.
I was quite surprised and impressed when proof reading the manuscript, as I had not come across this use of acupuncture before. But I have learnt not to rely totally on my memory regarding the acupuncture literature, so I did a quick PubMed search. To my further surprise I discovered a published RCT on the subject,[2] a protocol for a further one,[3] and a retrospective case series of 20 patients from 2013.[4] How could I have missed all of those?
The RCT was based in Ningbo, China – a city directly south of Shanghai and separated from it by the Hangzhou bay. 60 patients admitted with aSAH were randomised to receive EA or mock TENS to GV20 (a point at the top of the head). Four sessions were performed over 2 weeks following endovascular coiling or surgical clipping of the offending aneurysm. EA was at 2Hz with an intensity that was gradually increased from 0 to 5mA. The sessions lasted 30 minutes.
As a side note, the deep somatic nerves stimulated by needles in the epicranial tissue at GV20 are likely to be carried to the spinal trigeminal nucleus by branches of the facial nerve innervating occipitalis or frontalis muscles. The skin at this site is in the C2 distribution, but skin stimulation is unlikely to be as important as the deeper tissue layer.
The paper measured a variety of blood flow parameters, but the most eye-catching result was the percentage of good outcomes on the Glasgow Outcome Score (GOS).
Glasgow Outcome Score:
- Death
- Persistent vegetative state
- Sever disability
- Moderate disability
- Low disability
The EA group scored 4 or 5 on the GOS at 3 months in 29 out of 30 patients, and the control group scored 4 or 5 in just 19 (p=0.001).
This is almost in the same category as EA preventing mice dying of septic shock![5,6] With figures like this we would be insisting on getting the treatment for one of our family unlucky enough to suffer an aSAH. Don’t you think?
References
1 Dietzel J, Eck T, Usichenko T. Treating Therapy-Resistant Headache After Aneurysmal Subarachnoid Hemorrhage with Acupuncture. Neurocrit Care Published Online First: 29 April 2019. doi:10.1007/s12028-019-00718-3
2 Sun J, Liu Y, Zhang J, et al. Electroacupuncture Improves Cerebral Vasospasm and Functional Outcome of Patients With Aneurysmal Subarachnoid Hemorrhage. Front Neurosci 2018;12:724. doi:10.3389/fnins.2018.00724
3 Cho S-Y, Lee D-H, Shin HS, et al. The efficacy and safety of acupuncture for cerebral vasospasm after subarachnoid hemorrhage: study protocol for a randomized controlled trial. Trials 2015;16:68. doi:10.1186/s13063-015-0591-7
4 Ko C-N, Lee I-W, Cho S-Y, et al. Acupuncture for Cerebral Vasospasm After Subarachnoid Hemorrhage: A Retrospective Case–Control Study. J Altern Complement Med 2013;19:471–3. doi:10.1089/acm.2012.0076
5 Torres-Rosas R, Yehia G, Peña G, et al. Dopamine mediates vagal modulation of the immune system by electroacupuncture. Nat Med 2014;20:291–5. doi:10.1038/nm.3479
6 Villegas-Bastida A, Torres-Rosas R, Arriaga-Pizano LA, et al. Electrical Stimulation at the ST36 Acupoint Protects against Sepsis Lethality and Reduces Serum TNF Levels through Vagus Nerve- and Catecholamine-Dependent Mechanisms. Evid Based Complement Alternat Med 2014;2014:451674. doi:10.1155/2014/451674

You must be logged in to post a comment.