
Inspired by Goebel et al 2021.[1]
FMS – fibromyalgia syndrome
key to acronyms
FM – fibromyalgia
IgG – immunoglobulin G
IF – impact factor
HC – healthy controls
CM – C-mechanoreceptor
CMC – cold-sensitive CM
DRGs – dorsal root ganglia
SGCs – satellite glial cells
MTrPs – myofascial trigger points
SHA – self home acupuncture
ST36 – an area in upper tibialis anterior (MC’s favourite)
ZP – Zongping (15 to 20mm below ST36 in the same muscle)
I have a had a running set of searches on PubMed for both myofascial pain and acupuncture for many years, and over the years I have got used to the fact that the myofascial pain search includes papers on FM. I scan the titles, but for the most part I ignore this literature unless it pops up on both simultaneously, and thus includes acupuncture as well as FM.
This paper only showed up the myofascial pain search, so normally I would pass over it. This time I was alerted to something special by a simultaneously listed editorial in the same journal.[2] This editorial was written by Kevin Tracey – a name I am very familiar with from the vagal anti-inflammatory reflex story.[3] The journal was not familiar to me, but it has been around for nearly a century and has an impressive IF (14.808).
I should warn you now that this paper has nothing to do with acupuncture, but if you are an acupuncture practitioner, and you ever see patients with FMS, this paper is relevant to you, since it has major implications for our understanding of the syndrome and will likely lead to future novel treatments for the condition. I will also suggest what the implications might be for optimum treatment of FMS with acupuncture below.
elegant reverse translational research
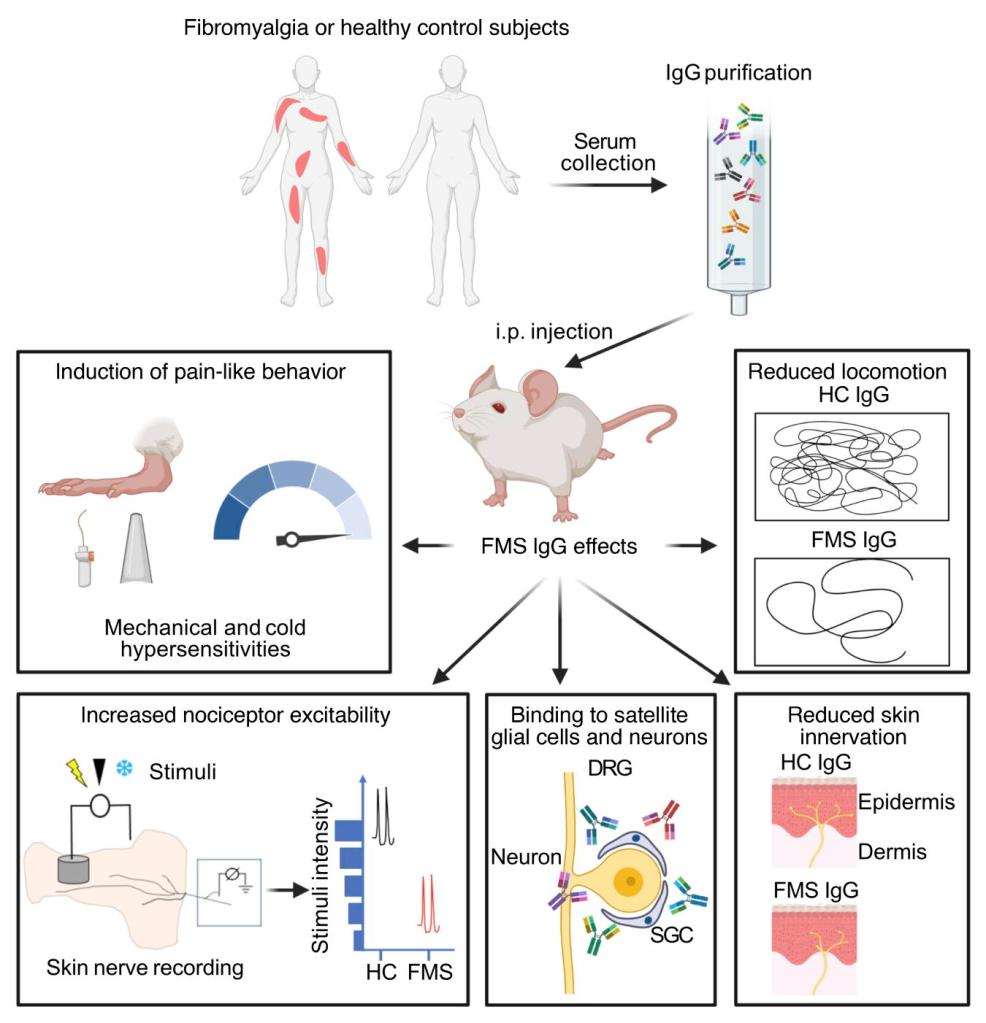
Goebel and colleagues performed some really elegant reverse translational research by using IgG in serum from human patients with FMS and creating a similar syndrome in mice injected with this serum. I have never heard of anything like this before, and the results are really surprising.
Mechanical and cold hypersensitivity was induced by IgG purified serum of individual FMS patients, but not by the equivalent serum from healthy subjects (HC), or FMS serum depleted of IgG. The abnormalities were also induced by pooled serum with each individual component being at too low a concentration to induce the changes alone. These changes lasted from 3 to 4 weeks after induction with FMS IgG-intact serum.
Locomotor activity was also affected in the FMS IgG mice compared with HC IgG.
Mechanical activations thresholds were reduced in Aδ- and C-mechanorecptors (CM) in preparations from mice treated with FMS IgG compared with HC IgG. Cold thresholds were not different, but the proportion of cold-sensitive CM units was increased, presumably mediating the increased cold sensitivity of the FMS IgG mice.
So, if peripheral afferents are more sensitive, are they directly affected by the FMS IgG? What has this got to do with a defect in central descending inhibition or chronic fatigue or emotional distress? Well, it is looking as though these aspects of FM are downstream of the primary abnormalities.
FMS IgG labels glial cells in the DRG
The next thing the team did was to look where the FMS IgG was binding and try to determine the likely targets. There was no significant IgG detected in the brain or spinal cord, but significant accumulation in DRGs. The majority of the labelling was near the surface of SGCs rather than the primary afferent neurones themselves; however, there was a little labelling close to the surface of neurones. Myelinated fibre tracts and a small number of macrophages and endothelial cells were also labelled in the DRGs, but no cells in the spinal cord.
FMS IgG appears to increase activity in SGCs in vivo, but not to increase systemic inflammation. This increased activation may be responsible for the increased nociceptor activity, since we already know that the role of certain glial cells includes this sort of neuronal activation.
Protein microarrays were used to investigate potential targets for the FMS IgG. No characteristic patterns of reactivity were found, and the increases mostly appeared in protein fragments related to intracellular components, so unlikely to be binding targets.
Finally, a histological feature that has been identified in humans with more severe FMS was also found in the FMS IgG mice after just 4 days – a reduction in intraepidermal nerve fibre density.
We have been focussing on abnormalities in the CNS in FM for decades, whilst a few lone voices have promoted the idea of the condition being driven peripherally. The latter voices may have been right, but perhaps not for the right reasons. Who would have guessed?
What does this mean for acupuncture treatment of FM patients?
What does this mean for acupuncture treatment of FM patients? If the primary abnormality relates to auto-reactive IgG activating SGCs in DRGs, then targeting peripheral soft tissue (eg MTrPs) or attempting to influence CNS activity may not be getting close enough. Perhaps we should be thinking more about immunomodulation, even though systemic inflammation appears to be absent.
I’m starting to think that my approach to prophylaxis of chronic inflammatory conditions may be closer to the mark, in which case we need to try treating patients 2 or 3 times a week, which in the UK would almost certainly mean using an SHA approach. I’m thinking red needles at ST36 and LI11 rather than EA here, although some may be ok with the ST36–ZP approach with 2Hz burst or 2/15Hz.
It’s all food for thought!
References
1 Goebel A, Krock E, Gentry C, et al. Passive transfer of fibromyalgia symptoms from patients to mice. J Clin Invest 2021;131:144201. doi:10.1172/JCI144201
2 Tracey KJ. From human to mouse and back offers hope for patients with fibromyalgia. J Clin Invest 2021;131:150382. doi:10.1172/JCI150382
3 Tracey KJ. The inflammatory reflex. Nature 2002;420:853–9. doi:10.1038/nature01321

You must be logged in to post a comment.