
Inspired by Hu et al 2021.[1]

PID – prolapsed intervertebral disc
key to acronyms
IMHO – in my humble opinion
MRI – magnetic resonance imaging
Over the years I have seen many patients with back pain, including those with the source of pain in the back that presents as pain somewhere in the leg. My main interest was always those with unilateral symptoms and near normal lumbar flexion, because a lot of these were muscle problems that responded very quickly, if not instantly, to needling.
As my practice population changed, I naturally saw more patients with problems that were more difficult to treat, including those for which my needles could not reach directly to the problem. I had to develop assessment methods to try to work out what was happening within the spinal canal.[2]
PID was first proposed by Schmorl
PID was first proposed by Schmorl of Dresden in 1925, apparently in retirement, whereupon he examined some 3000 vertebral columns.[3] He found 38% with PID: 15% backwards into the vertebral canal and 23% into the vertebral body. Sometime later Adams & Hutton began mechanically loading cadaveric discs to failure and describing his findings.[4] He subsequently summarised his research with colleague in a book I found to be remarkably useful: The Biomechanics of Back Pain.[5] This text clearly borrowed heavily in certain aspects from a prior text by Bogduk that is also highly recommended.[6]
If you don’t have access to either of these I can recommend Michael Adam’s summary article in Acupuncture in Medicine that I commissioned from him in 2004.[7]
The term used in everyday language is a ‘slipped disc’, which begs the idea that it could be slipped back into place. You do not have to spend too much time with the texts I have mentioned above to appreciate that the forces required to ‘slip’ the disc in the first place are so colossal that there is unlikely to be any way of getting the disc material back in place.
However, the ‘slipped’ or more properly termed ‘extruded’ disc material can disappear with time, and hence my interest in this recent paper. It is a case report of spontaneous regression of a large lumbar disc fragment following conservative management (acupuncture and massage) and time – in this case only 4 months.
Patients often ask me how long it will take to recover, and I often pick the number 8 to 9 months although I cannot recall where I first heard that figure. I was attracted to this paper because the authors reviewed all the cases of spontaneous regression of lumbar disc herniation they could find in the literature and classified them according to whether the disc was classed as extruded or sequestered.
It is probably time to clear up the terminology isn’t it!
- Protrusion – a bulging of the annulus fibrosus but no herniation of the nucleus pulposus
- Herniation – some material from the nucleus passes through a defect in the annulus but not necessarily beyond the limit of the outer annulus
- Extrusion – some material from the nucleus herniates outside of the outer annulus
- Sequestration – some material from the nucleus herniates outside of the outer annulus and becomes separated from the rest of the nucleus pulposus
Average in months to PID regression 10.1
– extrusions 14.4
– sequestrations 6.8
Of the 32 cases of spontaneous regression included in the paper’s review, the average time until regression was noted was 10.1 months. But this time reduced to 6.8 months when only the sequestrations were included and rose to 14.4 months when only the extrusions were included.
The paper considered the different proposed mechanisms for spontaneous regression, but the only credible one they included (IMHO) was resorption through enzymatic degradation and phagocytosis.
rim enhancement on post-gadolinium T1–weighted MRI
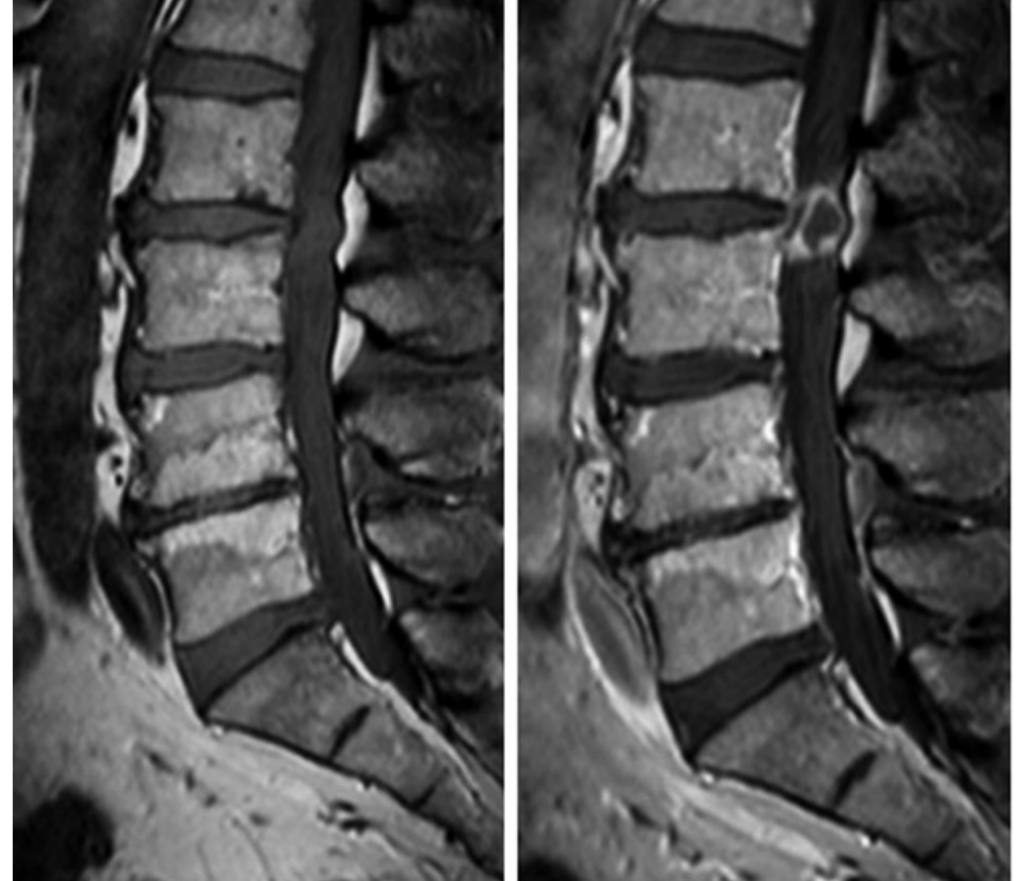
The authors suggest that rim enhancement of the sequestered disc material on post-gadolinium T1–weighted MRI could be a sign of more likely regression and therefore indicate a good response to conservative treatment. I think this is a very reasonable suggestion and a previous prospective observation study from Germany provides some histological support for this suggestion.[8]
References
1 Hu C, Lin B, Li Z, et al. Spontaneous regression of a large sequestered lumbar disc herniation: a case report and literature review. J Int Med Res 2021;49:3000605211058987. doi:10.1177/03000605211058987
2 Cummings M. Low back pain assessment for the medical acupuncturist. Acupunct Med 2004;22:189–202.
3 Leigh AD. The prolapsed intervertebral disc. Postgrad Med J 1947;23:141–50. doi:10.1136/pgmj.23.257.141
4 Adams MA, Hutton WC. The mechanics of prolapsed intervertebral disc. Int Orthop 1982;6:249–53. doi:10.1007/BF00267146
5 Adams MA, Bogduk N, Burton K, et al. The Biomechanics of Back Pain. Edinburgh: Churchill Livingstone 2002.
6 Bogduk N. Clinical anatomy of the lumbar spine and sacrum. Edinburgh: Chirchill Livindstone 1997.
7 Adams MA. Biomechanics of back pain. Acupunct Med 2004;22:178–88. doi:10.1136/aim.22.4.178
8 Löhr M, Lebenheim L, Berg F, et al. Gadolinium enhancement in newly diagnosed patients with lumbar disc herniations are associated with inflammatory peridiscal tissue reactions –evidence of fragment degradation? Clin Neurol Neurosurg 2014;119:28–34. doi:10.1016/j.clineuro.2014.01.008

You must be logged in to post a comment.