
Inspired by Chen et al 2022.[1]
FABP2 – fatty acid binding protein 2
key to acronyms
FSH – follicle stimulating hormone
hs-CRP – high sensitivity C-reactive protein
TNF-α – tumour necrosis factor alpha
IP10 – interferon-inducible protein 10
MCP-1 – monocyte chemoattractant protein 1
This week I am highlighting a paper that came up on my searches but does not involve acupuncture as a treatment or myofascial pain as a topic. It came up because one of the authors has the word ‘acupuncture’ in one of his affiliation addresses. So, essentially it came up by chance. The title intrigued me, and Plos One is a respected open access journal, so I had a look. The findings have implications for practice and since many readers will treat hot flushes with acupuncture, I thought it would be useful to highlight the paper.
It is a cross-sectional study including 289 postmenopausal women of 40 to 65 years of age. Postmenopausal was defined as the time after which women had experienced 12 consecutive months of amenorrhoea. They were divided into 4 groups based on the severity of hot flush symptoms:
- HF0 – never experienced hot flushes (n=117)
- HFm – mild hot flushes (n=33)
- HFM – moderate hot flushes (n=41)
- HFS – severe hot flushes (n=98)
From the introduction of this paper, I was reminded that, in postmenopausal women, hot flushes are associated with low grade systemic inflammation; and I learned that oestrogen affects the microbiome and increases gut epithelial integrity.
The women in this study were thoroughly weighed and measured… mostly measured using blood tests for a variety of factors: FSH, oestradiol, fasting glucose, haemoglobin, lipid profile, zonulin, FABP2, endotoxin, hs-CRP, TNF-α, IP10, and MCP-1.
Severity of hot flushes was positively correlated with FABP2, endotoxin, hs-CRP, TNF-α, and IP10. There was a significant difference between the 4 groups in circulating FABP2, endotoxin, hs-CRP, and TNF-α, but not in zonulin.
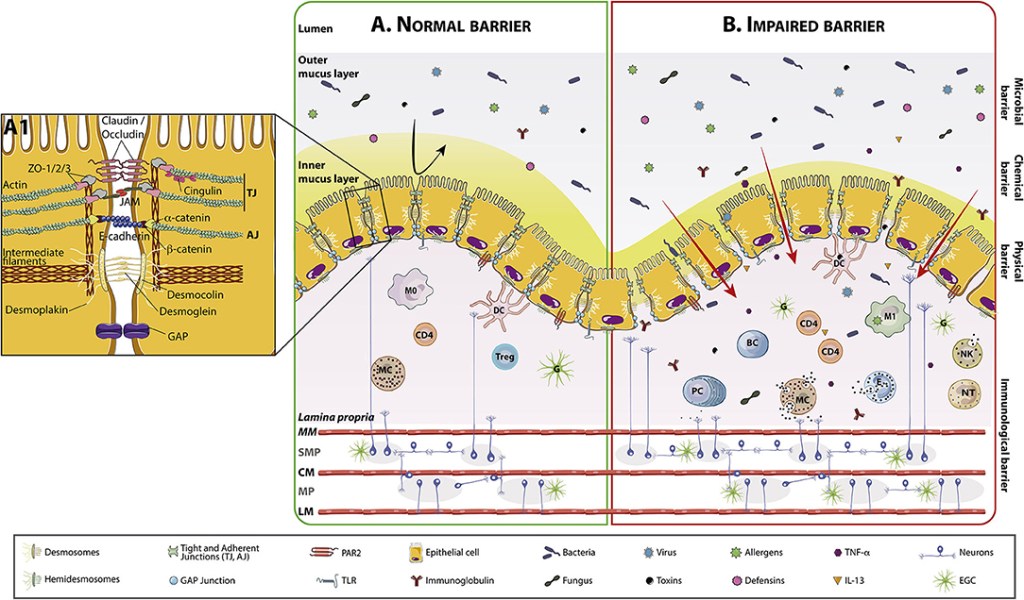
Zonulin is a physiological modulator of the intercellular tight junctions in the intestinal tract. It increases the permeability of these junctions and is the mammalian analogue of a toxin secreted by the cholera pathogen Vibrio cholerae.
FABP2 and zonulin are biomarkers that indicate the status of impaired intestinal permeability, so you would expect them both to correlate positively with hot flush severity. The authors suggest that the reason this was not the case here relates to the assay for zonulin not being specific to the intestine-derived factor, and the fact that zonulin is produced in other places, such as the liver and adipose tissue.
So, in this case FABP2 is a more sensitive marker for intestinal barrier function and it correlates positively with hot flush severity.
What does that mean for acupuncturists? Well, we already know that acupuncture can positively modify the intestinal microbiome, but more importantly we can give additional nutritional guidance directed at improving the intestinal barrier.
There is a lot of choice here but prebiotic dietary fibre and probiotic rich foods and supplements will be high up the list, and there is already a link to one product that proved useful in recovery from COVID on the blog: The UK Phyto-V trial.
Other dietary components include minerals, vitamins, nutraceuticals, amino acids, and short chain fatty acids. There are many other potential modifiers, and I found a useful review paper from 2021 in Frontiers in Nutrition.[2]
References
1 Chen T-Y, Huang W-Y, Liu K-H, et al. The relationship between hot flashes and fatty acid binding protein 2 in postmenopausal women. PloS One 2022;17:e0276391. doi:10.1371/journal.pone.0276391
2 Fortea M, Albert-Bayo M, Abril-Gil M, et al. Present and Future Therapeutic Approaches to Barrier Dysfunction. Front Nutr 2021;8:718093. doi:10.3389/fnut.2021.718093

You must be logged in to post a comment.