
Inspired by Wang et al 2022.[1]
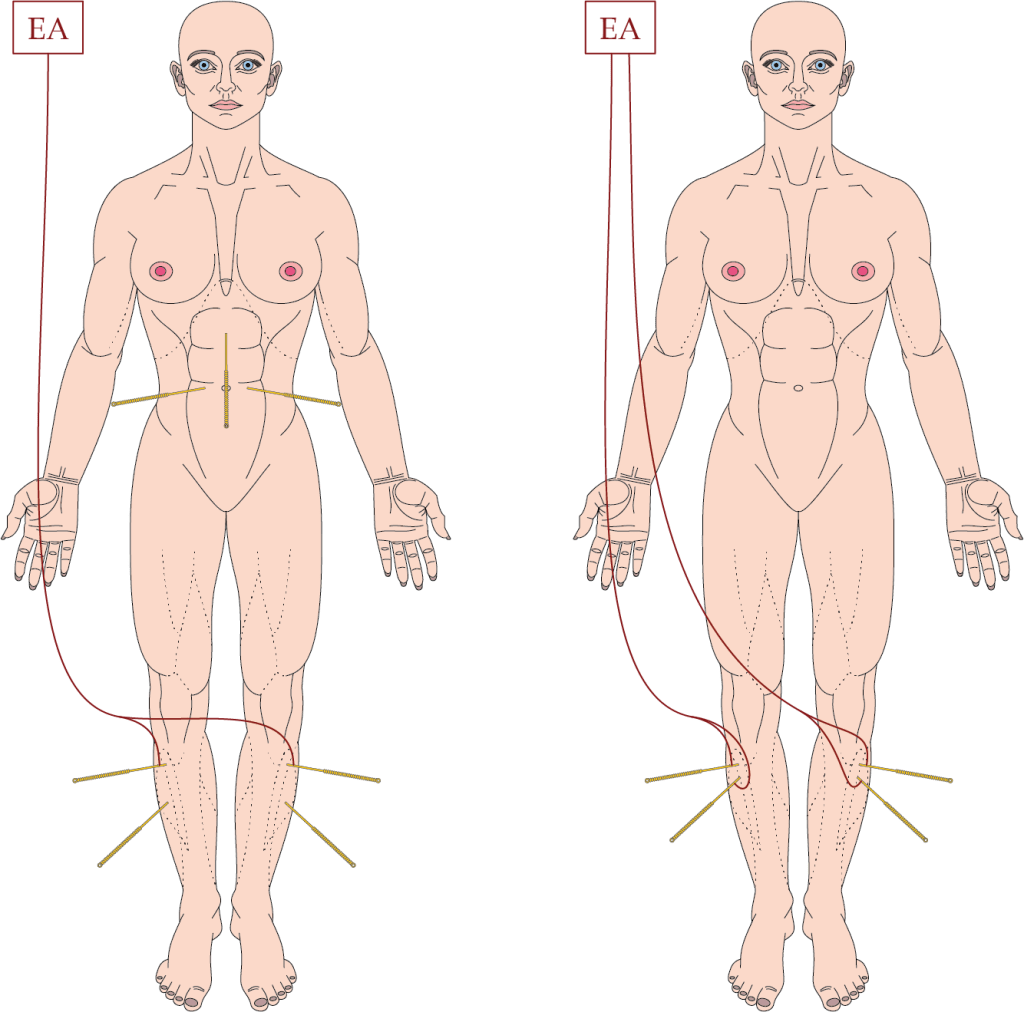
EA protocol used in Wang et al 2022 (left), and what I would do in the same circumstances (right).
EA – electroacupuncture
key to acronyms
ERAS – enhanced recovery after surgery
POI – postoperative ileus
MA – manual acupuncture
TEAS – transcutaneous electrical acupoint stimulation (a form of TENS)
TTNS – transcutaneous tibial nerve stimulation (a form of TENS)
TENS – transcutaneous electrical nerve stimulation
PONV – postoperative nausea and vomiting
Just published online on the 2nd November in JAMA Surgery, this paper was an obvious choice for the blog. We have long known of the role of acupuncture in stimulating bowel activity, indeed the famous report by James Reston in The New York Times was of treatment for his pain and POI following an appendicectomy.
This is a relatively large (n=249) sham controlled trial of EA for POI after laparoscopic resection of colorectal cancer. MA was performed at 3 abdominal points – CV12 and ST25 bilaterally. EA was applied across ST36, and MA was applied at ST37. Obviously, if I had been there, I would have connected ST36 to ST37 bilaterally and applied EA to both points, controlling the intensity of each leg separately, and dropped the abdominal needling completely.
Sham acupuncture involved superficial off-point needling without manual stimulation to 4 points, 2 of which were connected to an inactivated EA device. The sham points were all very close to the points used in the EA group.
Patients received 30 minutes of EA or sham daily for 4 consecutive days postop. Everyone was masked apart from the acupuncturists, and there was an assessment of blinding as well as credibility and expectation after the first session. The primary outcome was the time to first defaecation.
The patients in the EA group achieved the primary outcome 8 to 9 hours sooner on average than those in the minimal needling sham EA group. There were significant improvements in most related secondary outcomes; however, the trend in favour of a reduced hospital stay did not reach significance.
The ERAS experts who wrote in an invited commentary alongside the highlighted paper considered the results interesting but were cautious about what they referred to as the rather long time to bowel movements after laparoscopic surgery (3 days).[2] I tried desperately to find a paper that gave normative data on this following laparoscopic bowel resection but failed. Instead, I found a paper on interoperative hypothermia and POI (hypothermia should be avoided),[3] one on T regulator lymphocyte levels (higher is better and associated with a lower rate of POI),[4] the effect of TEAS at ST36,[5] and the effect of TTNS,[6] all in patients having laparoscopic colorectal cancer resections.
Finally, I found a paper suggesting that it was hard to achieve full compliance with ERAS in China.[7] This paper found that an incomplete ERAS protocol (less than 70% compliance) was associated with improved outcomes. The fact that this research was performed at all does validate the suggestion from the authors of the invited commentary that compliance with ERAS may have been the reason for the slightly longer than expected time to first defaecation in both groups.
The ERAS Society recommendations for colorectal surgery were first published in 2005 and as of 2018 are in their 4th iteration.[8] They are quite extensive, with 24 items, and range from prehabilitation and preoperative nutrition to prevention of PONV and POI. There is a very brief mention of the use of alternative therapies (including acupuncture) for PONV, but I was horrified to see the use of gabapentinoids mentioned as well.
References
1 Wang Y, Yang J-W, Yan S-Y, et al. Electroacupuncture vs Sham Electroacupuncture in the Treatment of Postoperative Ileus After Laparoscopic Surgery for Colorectal Cancer: A Multicenter, Randomized Clinical Trial. JAMA Surg Published Online First: 2 November 2022. doi:10.1001/jamasurg.2022.5674
2 Ljungqvist O, de Boer HD. Will Acupuncture Be the Next Addition to Enhanced Recovery After Surgery Protocols? JAMA Surg Published Online First: 2 November 2022. doi:10.1001/jamasurg.2022.5683
3 Choi J-W, Kim D-K, Kim J-K, et al. A retrospective analysis on the relationship between intraoperative hypothermia and postoperative ileus after laparoscopic colorectal surgery. PloS One 2018;13:e0190711. doi:10.1371/journal.pone.0190711
4 Wang H, Wang Y, Xing H, et al. Laparoscopic Surgery Within an Enhanced Recovery after Surgery (ERAS) Protocol Reduced Postoperative Ileus by Increasing Postoperative Treg Levels in Patients with Right-Side Colon Carcinoma. Med Sci Monit 2018;24:7231–7. doi:10.12659/MSM.910817
5 Huang W, Long W, Xiao J, et al. Effect of electrically stimulating acupoint, Zusanli (ST 36), on patient’s recovery after laparoscopic colorectal cancer resection: a randomized controlled trial. J Tradit Chin Med 2019;39:433–9.
6 Martellucci J, Sturiale A, Alemanno G, et al. The role of tibial nerve stimulation for enhanced postoperative recovery after colorectal surgery: a double-blind, parallel-group, randomized controlled trial. Tech Coloproctology 2021;25:195–203. doi:10.1007/s10151-020-02347-x
7 Jian C, Zhou Z, Guan S, et al. Can an incomplete ERAS protocol reduce postoperative complications compared with conventional care in laparoscopic radical resection of colorectal cancer? A multicenter observational cohort and propensity score-matched analysis. Front Surg 2022;9:986010. doi:10.3389/fsurg.2022.986010
8 Gustafsson UO, Scott MJ, Hubner M, et al. Guidelines for Perioperative Care in Elective Colorectal Surgery: Enhanced Recovery After Surgery (ERAS®) Society Recommendations: 2018. World J Surg 2019;43:659–95. doi:10.1007/s00268-018-4844-y

One thought on “EA for ERAS 2022”
Comments are closed.