
Stimulated by Wang et al 2023.[1]
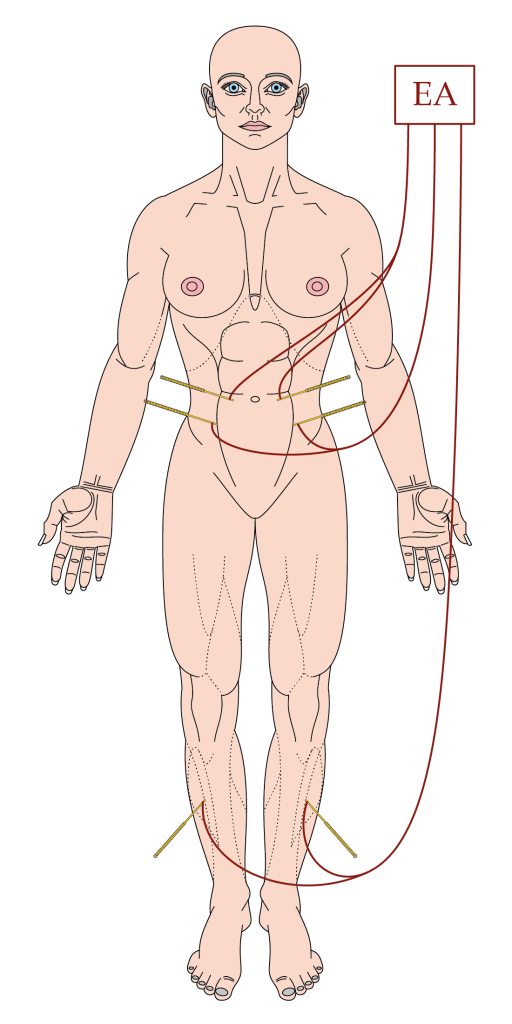
Diagram by MC.
EA – electroacupuncture
key to acronyms
OIC – opioid-induced constipation
CSFC – chronic severe functional constipation
5-HT – 5-hydroxytryptamine (serotonin)
TEAS – TENS applied to acupuncture points (ie TENS)
TENS – transcutaneous electrical nerve stimulation
SCC – severe chronic constipation
CSBM – complete spontaneous bowel movement
SBM – spontaneous bowel movement
The last author on this paper,[1] Zhishun Liu, that is just out in JAMA Network Open, was the first author on the very large (n=1075) sham controlled trial of EA on chronic severe functional constipation published in Annals of Internal Medicine in 2016.[2] He followed that up with a large (n=560) non-inferiority trial against prucalopride (a 5-HT4 receptor agonist with potent enterokinetic effects).[3] So, those two papers put EA on the map as a legitimate treatment in constipation.
This most recent trial is smaller (n=100) than the prior two, and it addresses OIC in patients with cancer, a very important side effect of medication that is commonly used in this population. A meta-analysis published in 2021 suggested the effectiveness of EA and EA like interventions (TEAS or TENS) in OIC, but did not include any sham controlled trials.[4]
Like the first very large trial on functional constipation, this was a sham controlled trial of EA. However, whilst the EA and sham interventions were very similar, there was a subtle difference in that 30 seconds of real EA stimulation was used at very low intensity (0.1mA to 0.2mA) in the sham group of the current trial. Sham EA was performed at points 2cm lateral to the real point locations and insertion was 2 to 3mm in depth with no manual stimulation.
The real EA stimulation was performed at points in the abdominal wall musculature (ST25 and SP14) and at a point in tibialis anterior (ST37). I think the points were attached across the midline, which is something I do not recommend in practice, but it would be unlikely to affect the results to any degree. This time 10Hz was used rather than 10/50Hz, and the intensity was set to the individual patient’s level of comfort between 0.5 and 4mA. Previously 0.1 to 1mA was reportedly used; this is something I commented on in the related blog (EA for CSFC) as being potentially subthreshold for many individuals. These changes are both sensible.
I illustrated the treatment protocol in the blog: EA vs Prucalopride in SCC. More importantly, in the current trial on OIC, EA was applied at ST37 as well, whereas previously manual stimulation alone was used at this point in tibialis anterior.
The same EA device was used in both studies, and I looked up the waveform parameters online. The pulse width was stated to be 0.2ms, which is similar to the devices I am used to using in clinical practice, so my comment on 1mA being potentially subthreshold still stands.
The primary outcome was also altered from the change in CSBM per week compared with baseline (during weeks 1 to 8) to the proportion of responders defined as those having at least 3 SBMs per week. This change certainly makes the results appear more impressive in the abstract, with the EA group coming in at 40.1% and the sham group 9.0% at week 8 (end of treatment phase).
SBM results looked similar to those in the previous very large sham controlled trial, apart from the baseline being much lower in the latter (0.5 CSBM versus 1.5 SBM). Obviously the ‘C’ is different here, and I guess this comes down to how the patient rates a SBM to be ‘complete’ or not on their diary. In the current trial, SBMs improved from 1.5 per week to just over 3 per week in the EA group, and in the larger trial, CSBMs increased from just under 0.5 per week to nearly 3 per week.
Well, this is another well conducted and reported RCT of EA in constipation and the first sham controlled RCT in OIC. The authors conclude that:
This randomized clinical trial found that 8-week EA treatment could increase weekly SBMs with a good safety profile and improve quality of life for the treatment of OIC. Electroacupuncture thus provided an alternative option for OIC in adult patients with cancer.
Wang et al 2023.[1]
I should just temper that conclusion for readers in the West with the reminder that 24 sessions of 30 minutes EA were provided for each patient in an 8-week period. That is 3 sessions per week for 2 months. The larger trial from 2016 managed 28 sessions in 8 weeks by filling in the missing days in the first 2 weeks of a 3 session a week schedule (ie daily weekday sessions for the first 2 weeks).
References
1 Wang W, Liu Y, Yang X, et al. Effects of Electroacupuncture for Opioid-Induced Constipation in Patients With Cancer in China: A Randomized Clinical Trial. JAMA Netw Open 2023;6:e230310. doi:10.1001/jamanetworkopen.2023.0310
2 Liu Z, Yan S, Wu J, et al. Acupuncture for Chronic Severe Functional Constipation: A Randomized Trial. Ann Intern Med 2016;165:761–9. doi:10.7326/M15-3118
3 Liu B, Wu J, Yan S, et al. Electroacupuncture vs Prucalopride for Severe Chronic Constipation. Am J Gastroenterol Published Online First: December 2020. doi:10.14309/ajg.0000000000001050
4 Han C, Liu Y, Fan H, et al. Acupuncture Relieves Opioid-Induced Constipation in Clinical Cancer Therapy – A Meta-Analysis and Systematic Review. Clin Epidemiol 2021;13:907–19. doi:10.2147/CLEP.S324193

You must be logged in to post a comment.