
Inspired by Jin et al 2022.[1]
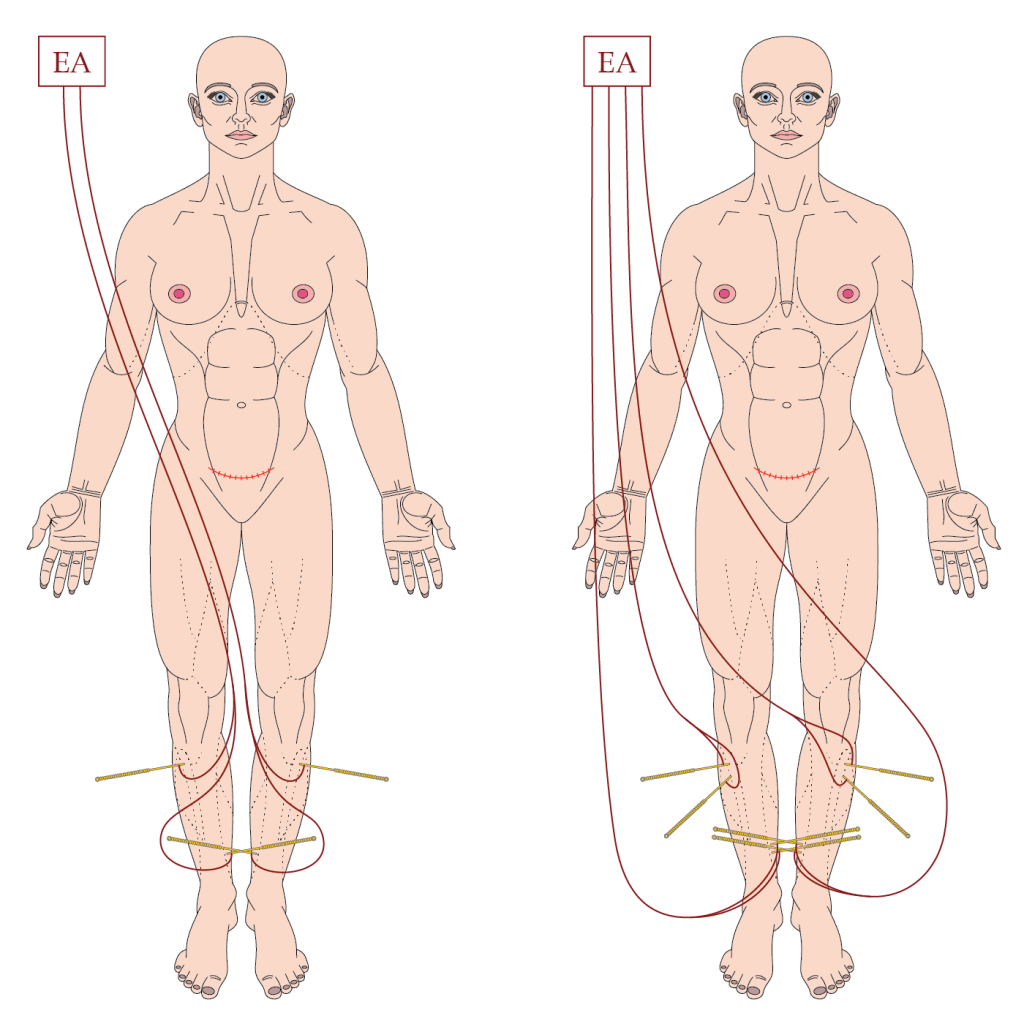
EA protocol used in Jin et al 2022 (left), and what I would do in the same circumstances (right).
EA – electroacupuncture
key to acronyms
CS – caesarean section
NAPC – number of analgesic pump compressions
PCIA – patient controlled intravenous analgesia
IL-6 – interleukin 6 (a proinflammatory cytokine)
TAP – tranversus abdominis plane
I noticed this paper because my friend Taras Usichenko has been involved in acupuncture for pain control after CS for some years and we recently published the RCT he led on the topic.[2] The current paper comes from Hangzhou, which has been mentioned on this blog a few times previously (SAH headache 2019, ST36 EA and antitumour effects 2021, Pudendal EA for LUTS 2021). This study is different in design in that it randomised women post-operatively rather than preoperatively, and used intermittent EA application rather than indwelling needles.
EA was applied post-op at 6, 12, 24 and 48 hours. Patients (n=158) were randomised to 2Hz EA, 20/100Hz EA or sham EA with blunt shorter needles (the so-called pragmatic placebo needle). Sessions were 25 minutes, and the intensity was set between 0.1 and 5.0mA depending on tolerance. We are not told about pulse width, but that is probably fixed and we are told about the device used.
The primary outcome was the NAPC at 48 hours. All patients had access to fentanyl via PCIA. Secondary outcomes were pain scores, fentanyl consumption at 48 hours, serum levels of IL-6 and procalcitonin at 24 and 48 hours, and time to first ‘exhaust’ (I assume that refers to flatus ie exhaust from the lower exit of the bowel).
NAPC was significantly lower in the groups receiving real EA, without any difference between the two frequencies. At 48 hours the median (IQR) was 9 (4.3, 12.0) in the sham group, 1.0 (0.0, 3.0) in the 2Hz EA group, and 1.0 (0.0, 4.5) in the 20/100Hz EA group. In both real EA groups, the median was 0.0 at 6, 12, and 24 hours. In the sham group over the same time intervals the NAPC was 1.0, 3.0, and 5.5.
Pain scores and fentanyl consumption at 48 hours were both significantly lower, with no substantial differences between the two EA groups. There was a trend in favour of the 2Hz EA group regarding fentanyl consumption, and this just reached significance at 24 hours. There was a smaller (non-significant) trend in the other direction for pain scores, but that probably simply reflects greater fentanyl consumption.
IL-6 and procalcitonin did not reveal any mechanistic insights on this occasion.
I have asked Taras what he thinks of the PCIA plus EA after CS approach, but I expect he will say that opioids are not recommended in Germany for post-op pain following CS. The pain scores were lower with this approach but I guess there are aspects to consider for mothers and their new neonates that may not benefit from an excess of fentanyl.
Addendum
So, I heard from Taras. He had not seen the paper as he had been spending all his spare time recently on frozen surfaces playing ice hockey! He had a quick look, and gave me a rundown on the latest techniques for pain relief following CS.
He says that a mix of fentanyl and lidocaine is feasible but that physicians in the West are very reluctant to use new drugs in peripartum women. In Canada, continuous intravenous lidocaine is apparently standard for abdominal surgery.
TAP blocks are very popular for relieving pain after CS, and in Russia, anaesthetists now simply place thin catheters within the CS wound and allow women to inject themselves with ropivacaine as required.
References
1 Jin Y, Yu X, Hu S, et al. Efficacy of Electroacupuncture Combined with Intravenous Patient-controlled Analgesia after Cesarean Section: A Randomized Clinical Trial. Am J Obstet Gynecol MFM 2022. doi:10.1016/j.ajogmf.2022.100826
2 Usichenko TI, Henkel BJ, Klausenitz C, et al. Effectiveness of Acupuncture for Pain Control After Cesarean Delivery: A Randomized Clinical Trial. JAMA Netw Open 2022;5:e220517. doi:10.1001/jamanetworkopen.2022.0517

You must be logged in to post a comment.