
This blog was first published on 2nd August 2018 on a BMJ blog, and re-posted here when the former post was expunged ;-).
Effect of Acupuncture on Joint Pain Related to Aromatase Inhibitors Among Women With Early-Stage Breast Cancer – Hershman et al JAMA 2018

A large rigorous and statistically positive trial published in a prestigious general medical journal,[1] and an increasingly familiar conclusion rings out – acupuncture is significantly better than sham, but the difference may not be of clinical significance. This was not the exact conclusion of Hershman et al, but the latter is similar to this common EBM (Evidence-Based Medicine) mantra, perhaps insisted upon by the JAMA editors.


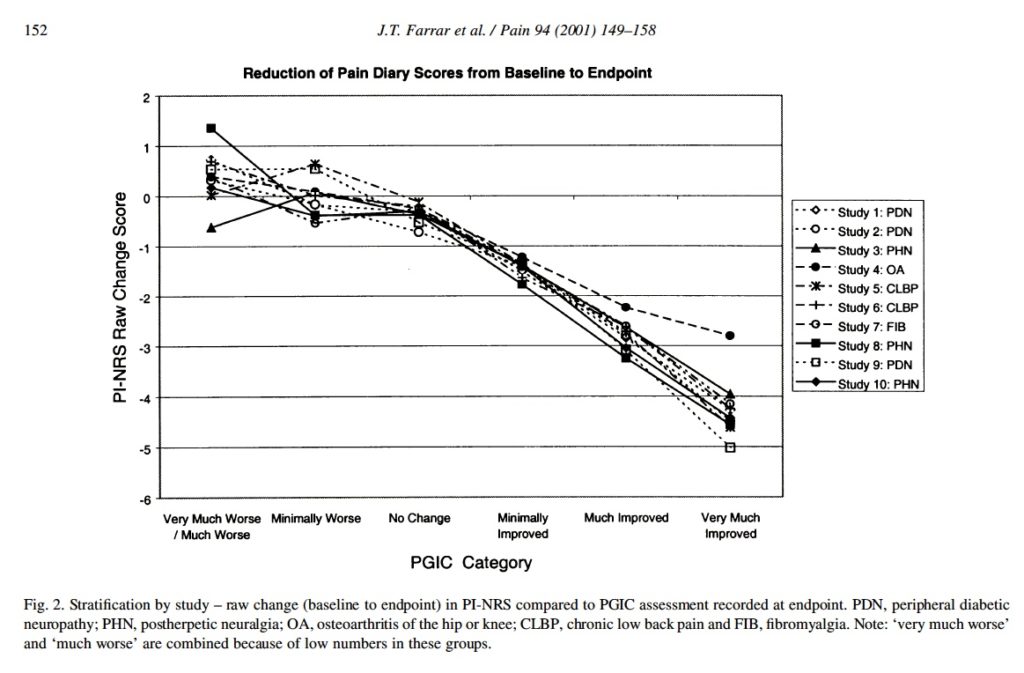
Hershman et al is the biggest trial of acupuncture for joint pain related to the use of aromatase inhibitors in women with breast cancer, and it randomised 226 women in a 2:1:1 split to verum (110), sham (59) or waitlist (57). The acupuncture protocols involved 18 sessions over 12 weeks, with 2 per week for the first 6 weeks. The primary outcome was the worst pain score on the Brief Pain Inventory (BPI-WP) at 6 weeks. The authors chose a clinically meaningful difference on this scale to be 2 points based on the analysis of 11-point Numerical Rating Scales (NRS) performed by Farrar et al.[2]
But is it a 2-point change from baseline that is clinically relevant, or a 2-point difference between groups? Well, the individual patient only knows the change from their own baseline, and the proportion of that change attributed to natural history or expectation in the group mean differences of a trial is irrelevant to the individual.
In the analysis by Farrar et al,[2] the change of 2 points considered to be clinically relevant was measured from baseline. In the present study by Hershman et al,[1] at the primary end point (6 weeks) the mean BPI-WP score in the acupuncture group had dropped 2.05 from baseline, and the percentage of patients with a drop of 2 points or more was 58%. This seems to be clinically relevant to me, but the conclusion reads:
“…the observed improvement was of uncertain clinical importance.”
At all time points the difference between acupuncture and sham control was statistically significant, but the difference did not reach 2 points, and this probably explains their conclusion. At first I assumed it was the JAMA editors that insisted on this conclusion, having seen this done before in a high profile general medical journal.[3] But having checked the protocol of Hershman et al,[1] I see that the authors have made the error of taking Farrar et al’s 2-points’ difference from baseline as a between group difference instead.
So I think this must be an error on the part of the authors rather than the insistence of the JAMA editors, but I expect it made it easier to publish the paper in this particular journal, based on its history of accepting negative acupuncture papers.
Whether this particular paper is considered positive or not, the data from it will inform future reviews, and currently these appear to be positive.[4,5]
Before I sign off on this blog, I should comment on the sham control group. It was a superficial penetrating off-point sham, and it did not seem to perform better than waiting list at 6 weeks, with the difference between acupuncture and sham at 0.92 and the difference between acupuncture and waiting list at 0.96. The effect of sham seemed to grow though, since at the 24-week point the difference between acupuncture and sham was only 0.59, and the difference between acupuncture and waiting list was 1.23.
Another pattern to note is that the difference between acupuncture and sham appeared smallest and not statistically significant for the outcome of pain interference, which is probably the closest of the outcomes used to health-related quality of life (HRQoL). Readers of this blog will be familiar with the finding from previous ‘big data’,[6] and my blog on the same.
References
- Hershman DL, Unger JM, Greenlee H, et al. Effect of Acupuncture vs Sham Acupuncture or Waitlist Control on Joint Pain Related to Aromatase Inhibitors Among Women With Early-Stage Breast Cancer: A Randomized Clinical Trial. JAMA 2018;320:167–76. doi:10.1001/jama.2018.8907
- Farrar JT, Young JP, LaMoreaux L, et al. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain 2001;94:149–58. doi:10.1016/S0304-3959(01)00349-9
- Brinkhaus B, Ortiz M, Witt CM, et al. Acupuncture in Patients With Seasonal Allergic Rhinitis. Ann Intern Med 2013;158:225. doi:10.7326/0003-4819-158-4-201302190-00002
- Chen L, Lin C-C, Huang T-W, et al. Effect of acupuncture on aromatase inhibitor-induced arthralgia in patients with breast cancer: A meta-analysis of randomized controlled trials. Breast 2017;33:132–8. doi:10.1016/j.breast.2017.03.015
- Halsey EJ, Xing M, Stockley RC. Acupuncture for joint symptoms related to aromatase inhibitor therapy in postmenopausal women with early-stage breast cancer: a narrative review. Acupunct Med 2015;33:188–95. doi:10.1136/acupmed-2014-010735
- Saramago P, Woods B, Weatherly H, et al. Methods for network meta-analysis of continuous outcomes using individual patient data: a case study in acupuncture for chronic pain. BMC Med Res Methodol 2016;16:131. doi:10.1186/s12874-016-0224-1

You must be logged in to post a comment.