
Stimulated by Astini & Riberto 2023.[1]
OA – osteoarthritis
key to acronyms
VAS – visual analogue score
WOMAC – Western Ontario and McMaster Universities Osteoarthritis Index
I am writing this blog from a nice big seat on an Iberia A350 from MAD to LHR. I was in Madrid for a Q&A session in an online acupuncture conference – my presentation was pre-recorded and translated. My title was acupuncture and placebo… a bit of an old chestnut, and indeed a rather similar topic to my first ever presentation in Spain just over 20 years ago.
One of the questions was about what practitioners can do in their acupuncture clinics in terms of research. My reply included keeping good records and evaluating outcomes without leaving any patients out, even if they were not treated. The second step might be to do what these authors have done in the paper I am highlighting this week – a single arm prospective cohort trial (other possible names could be prospective case series, or before-and-after study, or pre-post study).
This looks very similar to an outcomes audit or a service evaluation, but the difference is that a cohort trial with outcomes that are additional to those used in normal practice needs ethics approval and trial registration prior to recruitment.
The cohort in this case was patients with severe hip OA (n=12) and it was based in a place called Black Creek (Ribeirão Preto), which is about 3 days walk (300km) north (and slightly west) of São Paulo. I thought we (the BMAS journal – Acupuncture in Medicine) had an editorial board member from this place (JB), who I first met in Barcelona 15 years ago. But I was wrong, JB is from Black River (Rio Preto), which is a further 2 days walk (200km) west of Black Creek (Ribeirão Preto), so that is about 5 days walk from São Paulo. It is a one-hour flight, so I think I’ll do that when I go to visit him… I am overdue by several years!
This is a small cohort, but it is well measured and reported, and nobody was left out. When performing a prospective single-arm study like this it is important to capture good data at as many time points as you can, but especially before and after the intervention. Next most important is some sort of follow-up. In this case they remeasured at 5 weeks after acupuncture. Outcomes during the treatment course are not so important but can add some useful information about the trajectory of any response or change, and they are relatively easy to capture as you are seeing the patients for treatment.
In this study they used VAS pain, WOMAC, the 10m walk test, and the use of analgesics (medication diary). They measured VAS pain every week, but only recorded WOMAC at baseline, after treatment and at follow-up.
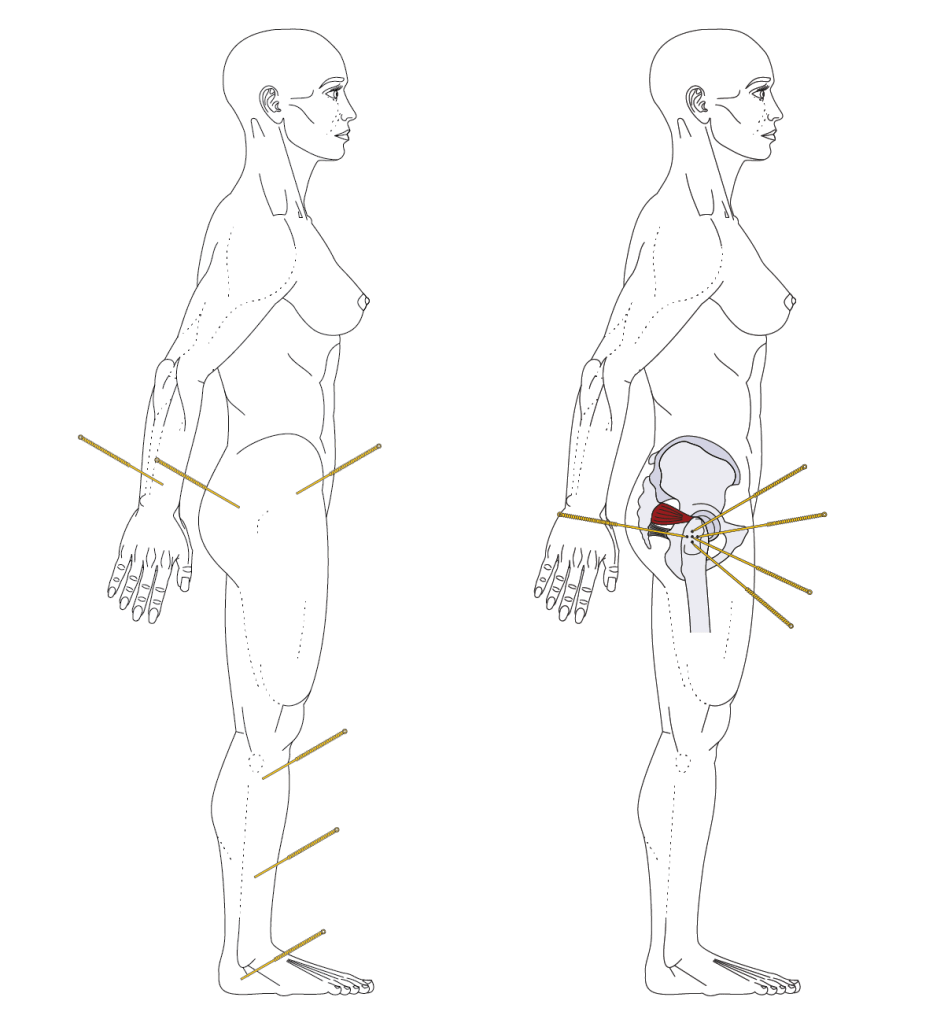
The acupuncture treatment involved 10 weekly sessions using 6 points and manual stimulation of 0.30x70mm needles (I am guessing they did not use 70mm for all the points – perhaps just the first 2 in the following list). The patients were treated in side-lying for 20 minutes, and the points used were: GB29, GB30, GB34, GB36, BL62, TE5.
VAS pain dropped from a mean of 75.8 in an almost linear trajectory over the 10 sessions to 20.0. The standard deviation was also around 20, meaning that at least 3 patients had no pain at all if the distribution was normal.
After 5 weeks the mean pain VAS had risen again to nearly 50, indicating that this population is likely to need regular top-ups.
The WOMAC results were similar, reducing from 74.7 to 45.7 and then back up to 54.6 at the 5-week follow-up.
There was a large reduction in the use of analgesic medication with most patients (8 of 12) not using any in the last week of the treatment course. The remining 4 patients reduced analgesic consumption by 70%.
The one thing I would have liked to have seen in this study was longer follow-up with the addition of monthly top-ups if this is to be considered as a viable strategy for long term management of hip OA.
There are only 2 sham controlled trials of acupuncture in hip OA,[2,3] and when pooled they do not demonstrate a statistically significant effect; however, the data is compatible with the possibility of a beneficial result of moderate effect size.[4]
The controls used in these 2 trials span the range from deep intramuscular needling away from classical acupuncture points and meridians to non-penetrating needling at the same points used for the verum acupuncture. Ironically, the mean group difference is slightly bigger in the trial comparing deep needling with deep needling!
References
1 Astini R, Riberto M. Acupuncture in the Treatment of a Series of Patients with Chronic Pain Associated with Hip Osteoarthritis. Rev Bras Ortop. 2023;58:e750–4.
2 Fink MG, Kunsebeck H, Wipperman B, et al. Non-specific effects of traditional Chinese acupuncture in osteoarthritis of the hip. Complement Ther Med. 2001;9:82–9.
3 White P, Bishop FL, Prescott P, et al. Practice, practitioner, or placebo? A multifactorial, mixed-methods randomized controlled trial of acupuncture. Pain. 2012;153:455–62.
4 Manheimer E, Cheng K, Wieland LS, et al. Acupuncture for hip osteoarthritis. Cochrane Database Syst Rev. 2018;5. doi: 10.1002/14651858.CD013010

You must be logged in to post a comment.