
Stimulated by Mao et al 2021.[1]
EA – electroacupuncture
key to acronyms
AA – auricular acupuncture
UC – usual care
PEACE – Personalised EA vs AA Comparative Effectiveness
MSK – musculoskeletal
MSKCC – Memorial Sloan Kettering Cancer Center
ARC – Acupuncture in Routine Care
BFA – battlefield acupuncture
BPI – brief pain inventory
VA – The United States Department of Veteran Affairs
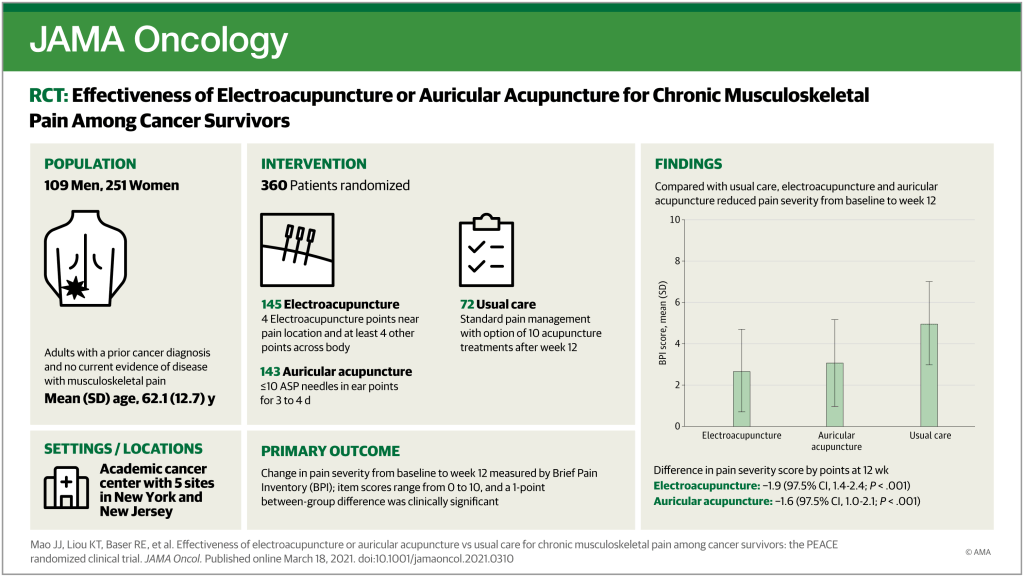
This is a large pragmatic trial based at MSKCC (n=360). The design has some similarities to the huge German ARC trials, which were part of the Modellvorhaben Akupunktur.[2] The population was cancer survivors suffering from chronic MSK pain.
There were 3 arms for the first 12 weeks, and 360 patients were randomised in a 2:2:1 ratio to EA, AA or usual care. 10 sessions of local EA at 2Hz were performed over 10 weeks. Four local points were used for the EA and 4 additional points were used to address other symptoms. The AA was actually the BFA protocol (see previous blog Ears and the battlefield), and ten sessions were provided. Usual care involved standard pain management approaches for chronic MSK pain, including analgesics, physical therapy and steroid injections. This group was offered a course of 10 sessions of acupuncture after the primary outcome was measured at 12 weeks. Hence the similarity with the ARC trials. A critical difference from the ARC studies was that this additional acupuncture treatment was not considered part of the trial, and no data is reported for this group beyond 12 weeks. This is a very good decision since both Cochrane and NICE have misinterpreted the 6-month data from ARC in the recent past. By not collecting or reporting this data, the authors have avoided this problem occurring with their trial in future meta-analyses.
The primary outcome was the change in average pain severity from baseline to week 12 measured using the BPI.[3] The BPI has 4 questions on pain severity, each of which is rated from 0 to 10.
- Worst pain in last 24 hours
- Least pain in last 24 hours
- Pain on average
- Pain right now
The BPI also has 7 items on pain interference, which are scored in the same way. These were used as one of the secondary outcomes in this trial.
Both EA and AA were associated with clinically relevant improvements in pain
Both EA and AA were associated with clinically relevant improvements (group mean change from baseline), but usual care was not so good, with a change of 0.48 on a 0 to 10 scale.
It is always tricky to ask more than one question in a clinical trial because statistical power will be different for different comparisons. This is why they used a 2:2:1 ratio. The smaller UC group was used as a comparator for each of the larger EA and AA groups, and the larger numbers in the active acupuncture groups allowed a more powerful comparison for the non-inferiority question.
As it turned out I was pleased to see that EA was significantly better than BFA in statistical terms. The paper does not say this because they posed a question on non-inferiority, but if you look at the CIs in the primary outcome change from baseline you will see that the BFA group mean does not reach the lower CI of the EA group and the authors state that non-inferiority of AA was not demonstrated.
The other difference between these groups was in terms of adverse events. Only 1 out of 145 patients discontinued EA because of an adverse event, but 15 out of 143 (10.5%) discontinued the BFA, mostly due to ear pain… I refer you back to the previous blog, and in particular the quote from the former US service woman:
“So, the VA has this treatment called battlefield acupuncture. Can confirm that my back doesn’t hurt anymore, but my ears sure as hell do!”
References
1 Mao JJ, Liou KT, Baser RE, et al. Effectiveness of Electroacupuncture or Auricular Acupuncture vs Usual Care for Chronic Musculoskeletal Pain Among Cancer Survivors: The PEACE Randomized Clinical Trial. JAMA Oncol Published Online First: 18 March 2021. doi:10.1001/jamaoncol.2021.0310
2 Cummings M. Modellvorhaben Akupunktur–a summary of the ART, ARC and GERAC trials. Acupunct Med 2009;27:26–30. doi:10.1136/aim.2008.000281
3 Cleeland CS, Ryan KM. Pain assessment: global use of the Brief Pain Inventory. Ann Acad Med Singapore 1994;23:129–38.

You must be logged in to post a comment.